
Using PDF files online can be a breeze with our PDF editor. You can fill in pa medical command form fillable here painlessly. To retain our tool on the leading edge of convenience, we aim to put into practice user-oriented features and enhancements on a regular basis. We're at all times pleased to get feedback - play a pivotal part in revampimg how we work with PDF forms. Here's what you will want to do to get going:
Step 1: Click the "Get Form" button at the top of this page to access our PDF tool.
Step 2: This tool gives you the ability to change your PDF form in various ways. Transform it by writing personalized text, adjust existing content, and put in a signature - all at your convenience!
So as to fill out this form, be certain to enter the information you need in every single blank field:
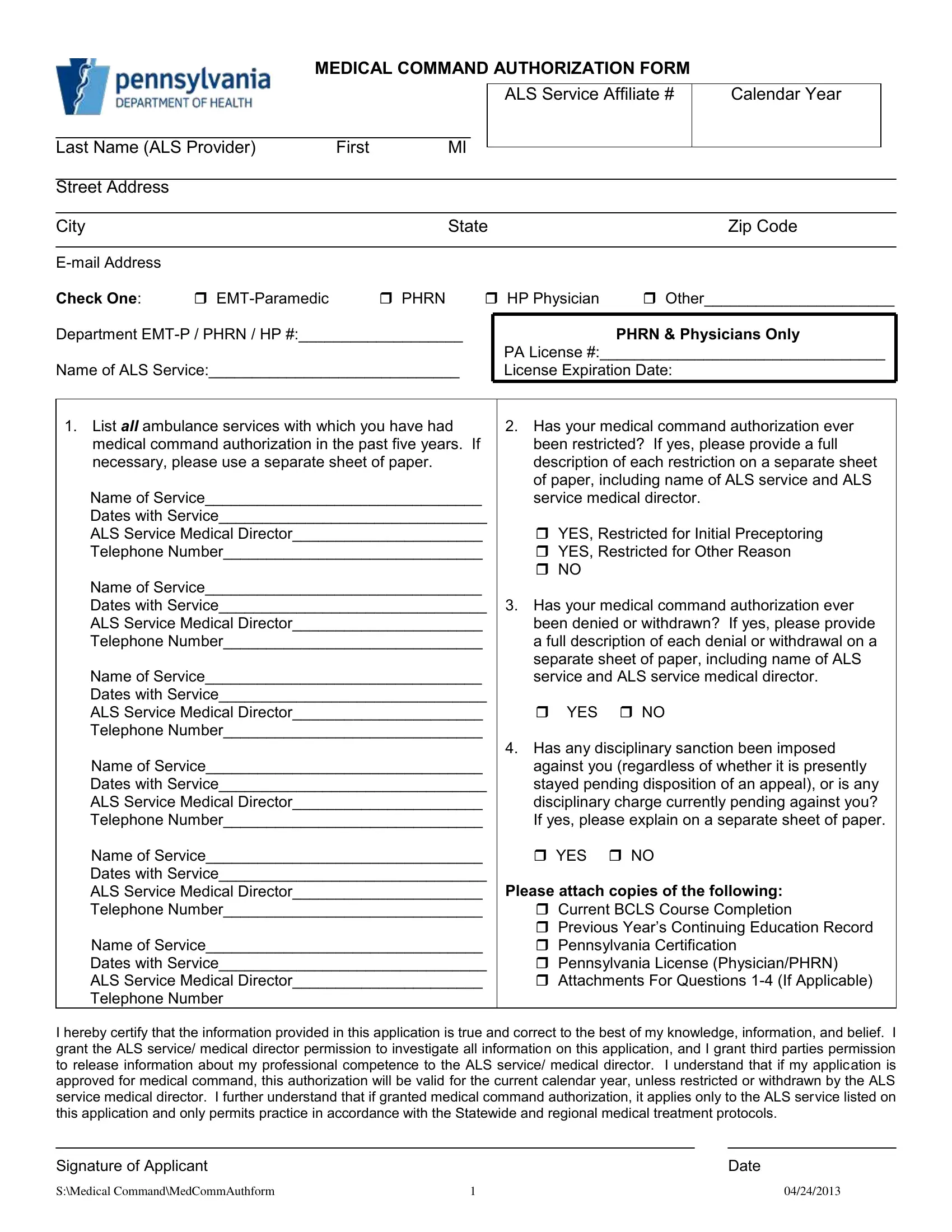
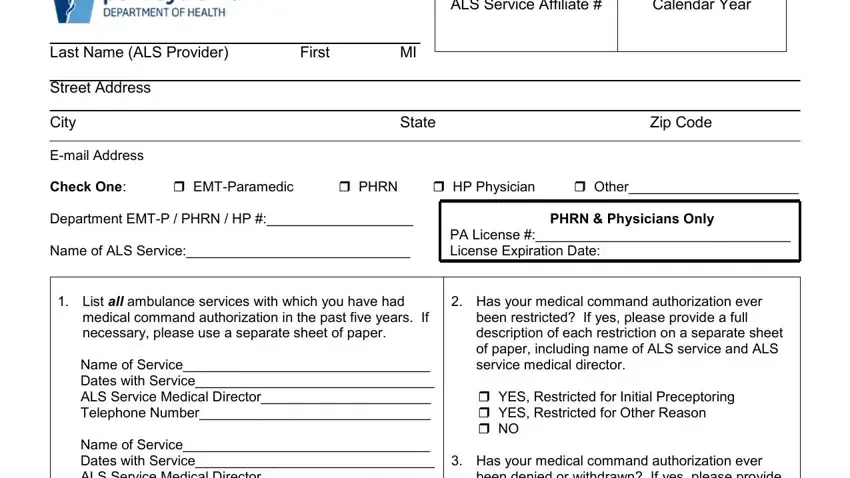
1. To start off, when filling in the pa medical command form fillable, start out with the area containing subsequent blank fields:
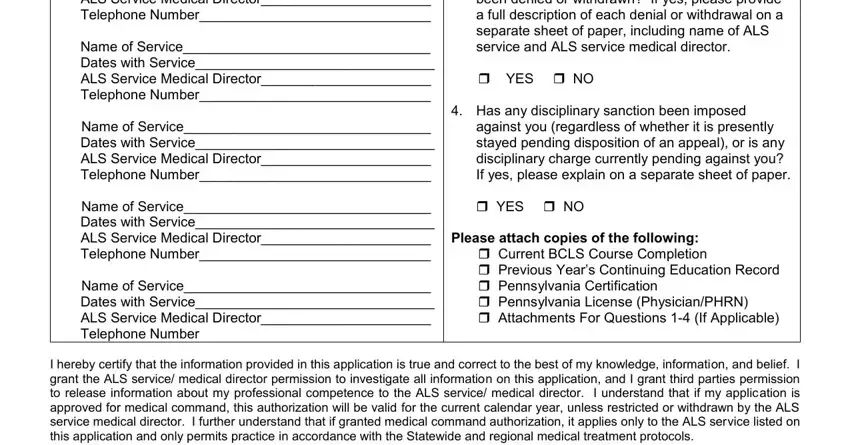
2. Given that this segment is completed, you're ready to insert the required details in Name of Service Dates with Service, Name of Service Dates with Service, Name of Service Dates with Service, Name of Service Dates with Service, been denied or withdrawn If yes, YES NO Has any disciplinary, against you regardless of whether, YES NO, Please attach copies of the, and I hereby certify that the so you're able to proceed to the 3rd part.
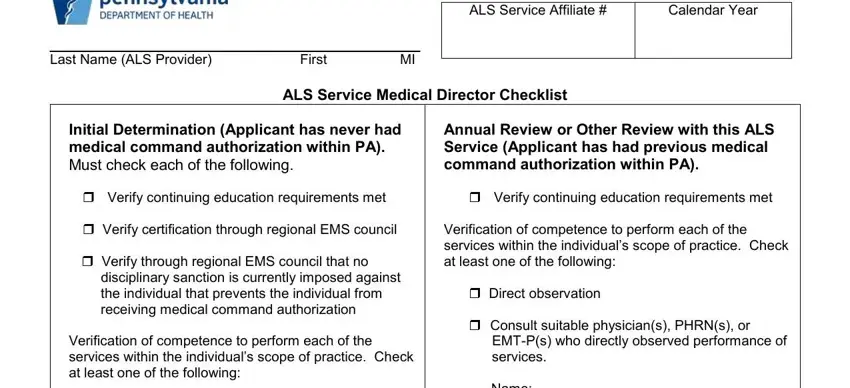
3. Throughout this part, have a look at Last Name ALS Provider, ALS Service Affiliate, Calendar Year, First, ALS Service Medical Director, Initial Determination Applicant, Verify continuing education, Verify through regional EMS, Annual Review or Other Review with, Verify continuing education, Verification of competence to, Direct observation, Consult suitable physicians PHRNs, and Name Name. Each one of these have to be completed with highest precision.
4. To move ahead, this next form section involves completing several empty form fields. Included in these are Direct observation, Consult suitable physician PHRN, Name Name, Name Name, Perform medical audit of records, Consult emergency department, Name Name, Consult medical command, Name Name, Consult ALS service medical, Name, Name, and Decision Rendered Choose Only One, which are vital to going forward with this particular PDF.
It's easy to make an error when filling out the Decision Rendered Choose Only One, hence ensure that you take another look before you'll finalize the form.
5. Because you draw near to the last parts of your file, you'll notice just a few more requirements that have to be met. Specifically, Initial with any ALS service, As the ALS service medical, Signature of ALS Service Medical, Signature of ALS Provider, Date, Date, and SMedical CommandMedCommAuthform must all be filled in.
Step 3: Make sure that the information is accurate and then press "Done" to progress further. Join us right now and instantly get access to pa medical command form fillable, ready for downloading. Each change you make is conveniently kept , so that you can customize the file at a later stage anytime. We don't sell or share the details that you enter while filling out documents at our site.