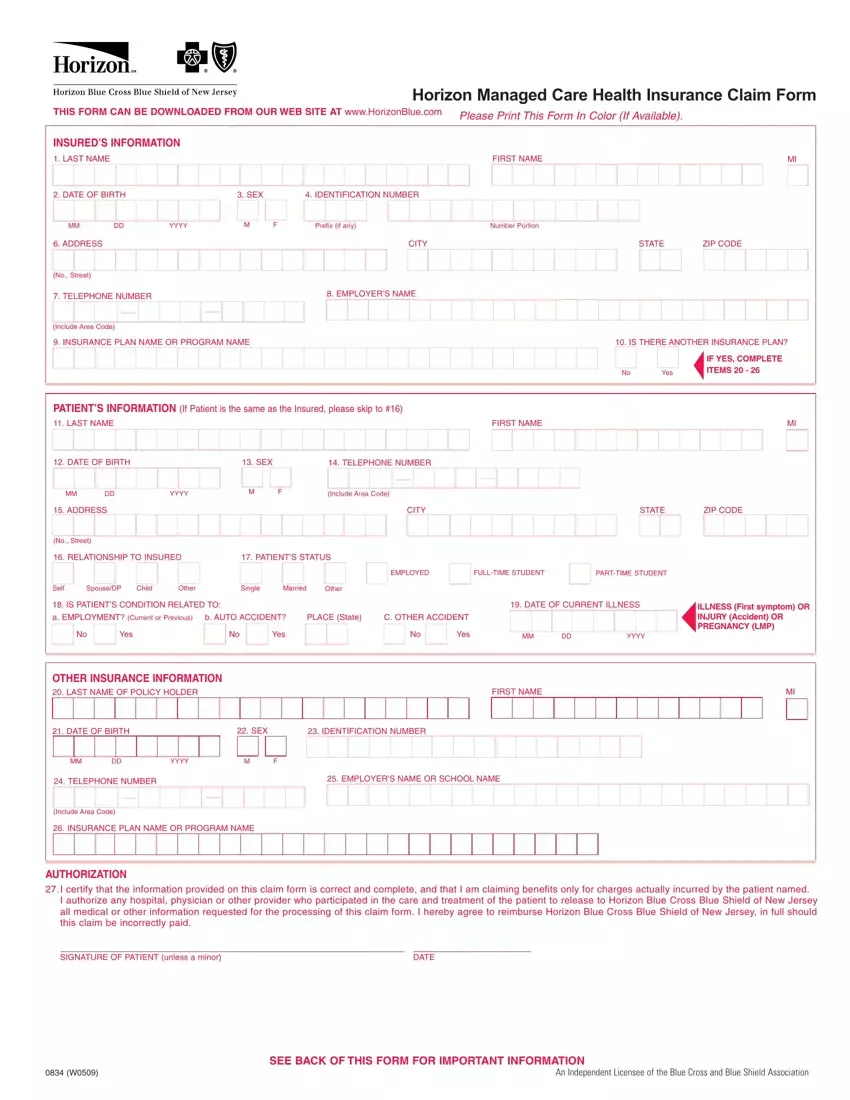
Navigating the landscape of health care claims can sometimes seem daunting, especially with the complex documentation required to ensure proper processing. The Horizon Managed Care Health Insurance Claim Form emerges as a crucial document for individuals seeking reimbursement or direct bill processing for medical services under the Horizon Blue Cross Blue Shield of New Jersey plan. This comprehensive form, available for download from the HorizonBlue website, mandates users to print in color—if possible—to improve clarity and facilitate the processing of their claims. Essential sections within the form capture both insured and patient information, ranging from basic identification data, such as names and dates of birth, to more detailed inquiries into the nature of the medical condition being claimed, whether it relates to employment, auto accidents, or other incidents. It also probes into other insurance coverage, underscoring the importance of coordination of benefits to ensure accurate claim settlement. Furthermore, an authorization section binds the claimant to the truthfulness of the provided information and allows for the release of necessary medical information to Horizon Blue Cross Blue Shield of New Jersey. The form is rounded off with instructions on submitting claims for more than one family member, what constitutes acceptable documentation, and the dire warnings against submitting fraudulent claims, illustrating the thoroughness expected in the claims process and the legal implications of misuse.
| Question | Answer |
|---|---|
| Form Name | Horizon Claim Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | horizon bcbs clain form, horizon claim form get, horizon claim form pdf, horizon claim form |
