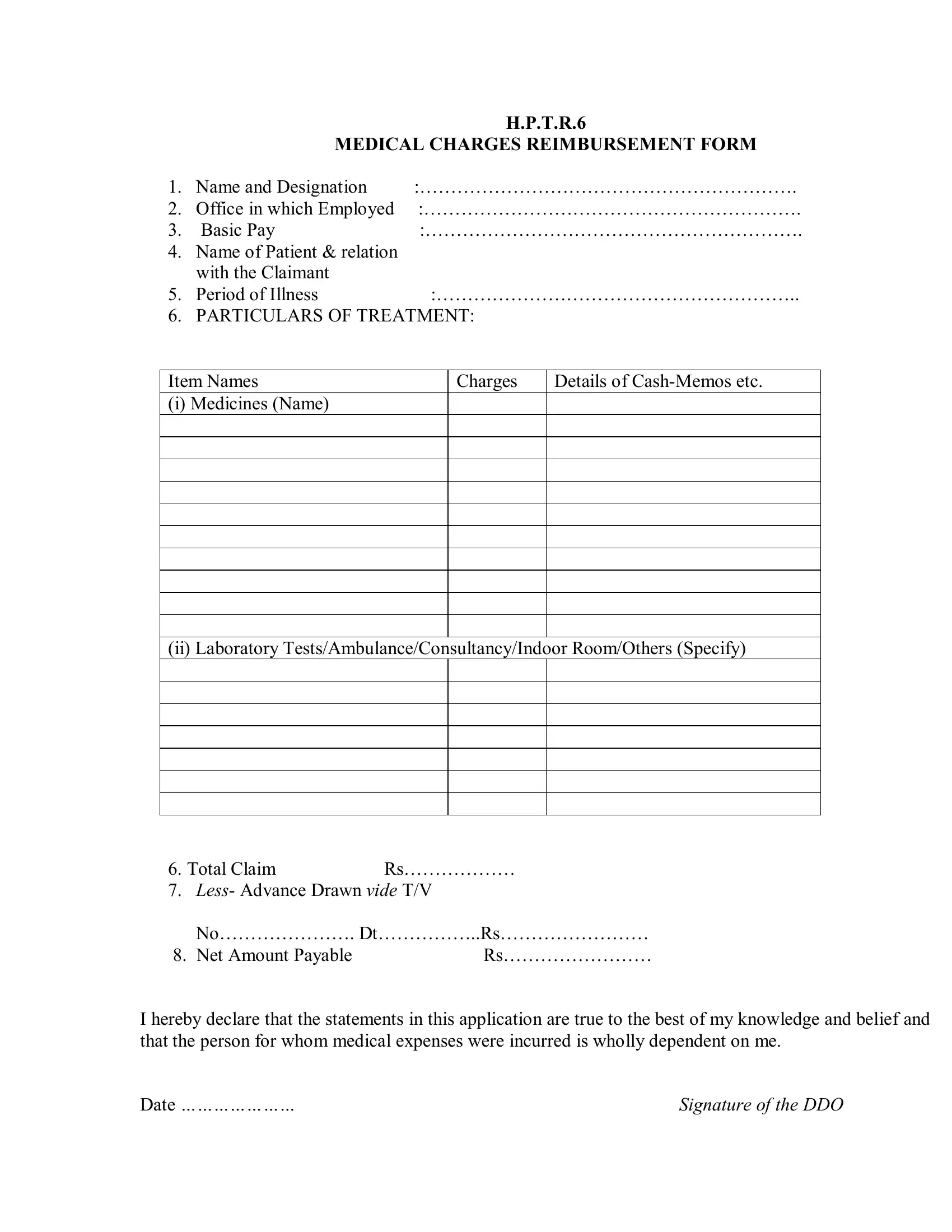
The H.P.T.R.6 form, a critical document for employees seeking medical charges reimbursement, embodies a structured approach to facilitate the process of claiming medical expenses incurred by individuals or their dependents. At its core, it requires comprehensive details such as the claimant's name, designation, office details, basic pay, and the relationship with the patient, ensuring a clear identification and authentication of the requestor. The form meticulously records the period of illness and provides a detailed section for outlining the particulars of the treatment, including medicines, laboratory tests, ambulance services, consultancy fees, indoor room charges among others, accompanied by the respective costs and supporting cash-memos. To further substantiate the claim, it meticulously asks for the total claim amount, adjustments for any advance drawn, and the net amount payable, encapsulating financial dynamics. A mandatory declaration by the claimant ensures the accuracy and truthfulness of the information provided, complemented by a verification certificate from a medical officer, who confirms the medical condition and treatment necessity. This procedure not only streamlines the reimbursement process but also implements checks to foster integrity and transparency. Additionally, the form outlines instructions about listing medicines and tests, attaching verified cash memos, and mentioning hospital admission details, guiding claimants through each step and ensuring that all necessary documentation is correctly compiled, making it an indispensable tool for managing medical reimbursement claims efficiently.
| Question | Answer |
|---|---|
| Form Name | H.P.T.R.6 Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 74 |
| Avg. time to fill out | 15 min 18 sec |
| Other names | medical reimbursement form pdf, hp medical reimbursement form, hptr6 online form, medical bill reimbursement form hp govt |
H.P.T.R.6
MEDICAL CHARGES REIMBURSEMENT FORM
1. |
Name and Designation |
:……………………………………………………. |
2. |
Office in which Employed |
:……………………………………………………. |
3. |
Basic Pay |
:……………………………………………………. |
4.Name of Patient & relation with the Claimant
5. |
Period of Illness |
:………………………………………………….. |
||
6. |
PARTICULARS OF TREATMENT: |
|||
|
|
|
|
|
Item Names |
|
Charges |
Details of |
|
(i) Medicines (Name) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(ii) Laboratory Tests/Ambulance/Consultancy/Indoor Room/Others (Specify)
6. Total Claim |
Rs……………… |
7. Less- Advance Drawn vide T/V |
|
No…………………. Dt……………..Rs…………………… |
|
8. Net Amount Payable |
Rs…………………… |
I hereby declare that the statements in this application are true to the best of my knowledge and belief and that the person for whom medical expenses were incurred is wholly dependent on me.
Date ………………… |
Signature of the DDO |
VARIFICATION CERTIFICATE
I, Dr …………………………. Hereby certify that ……………………………………………
Suffering from ………………………………….. and is /was under my treatment from ……………
To ……………………. And that the above mentioned medicines/ test were prescribed by me in this
connection.
This claim is verified for Rs………………………
Date…………………….. |
(Signature of Medical Officer) |
|
Designation & Seal |
|
|
Passed for Rs…………………(Rupees……………………………………………….)
And included in Bill No……………………………….Dated………………………….
(Signature of Controlling Officer) |
(Signature of the DDO) |
|
|
INSTRUCTIONS
1.List all the medicines, tests etc. individually.
2.Attach
3.Mention dates of admission to the Hospital, Stay etc.