Our PDF editor you are going to apply was made by our best software engineers. It is possible to prepare the 83039 form quickly and efficiently applying our software. Simply try out this specific guide to get going.
Step 1: Choose the orange "Get Form Now" button on the webpage.
Step 2: The form editing page is presently open. You can include information or manage existing details.
Create the 83039 PDF and enter the content for every single area:

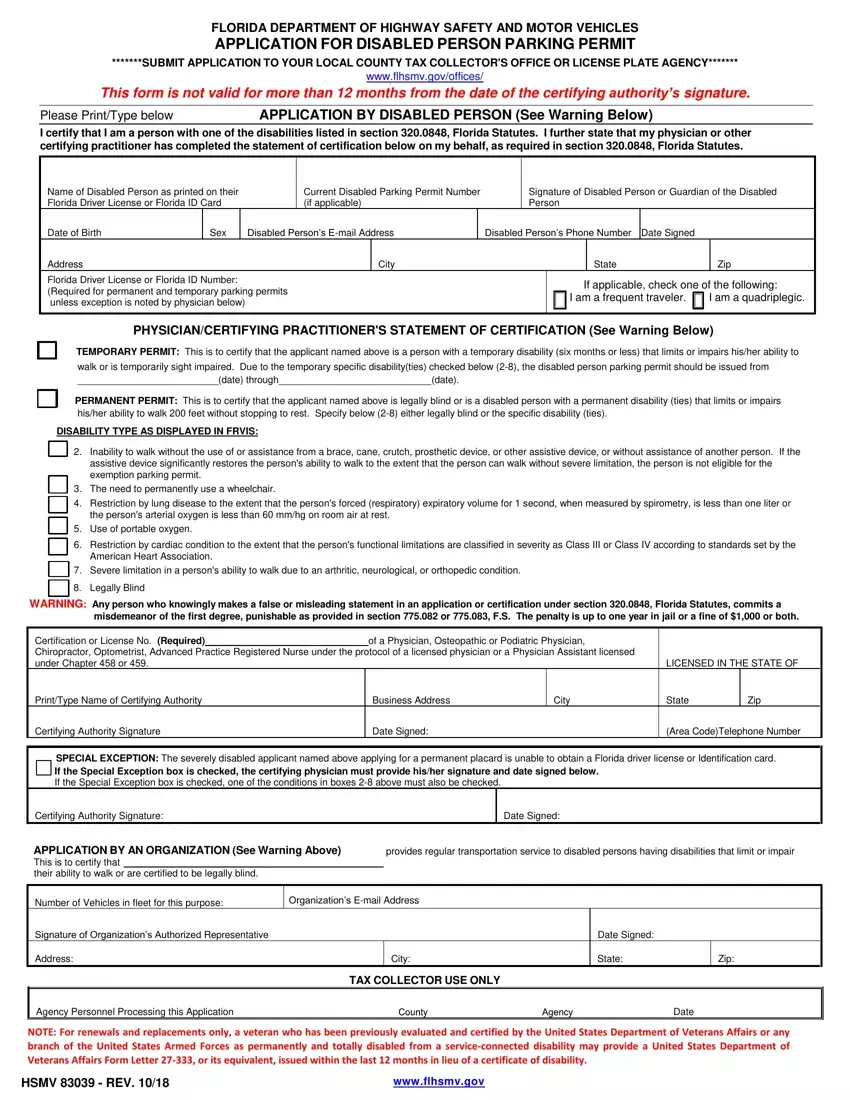
Jot down the details in the persons arterial oxygen is, Use of portable oxygen, Restriction by cardiac condition, American Heart Association, Severe limitation in a persons, Legally Blind, WARNING Any person who knowingly, misdemeanor of the first degree, Certification or License No, of a Physician Osteopathic or, LICENSED IN THE STATE OF, PrintType Name of Certifying, Business Address, City, and State.

Highlight the most important details of the Number of Vehicles in fleet for, Organizations Email Address, Signature of Organizations, Date Signed, Address, City, State, Zip, TAX COLLECTOR USE ONLY, Agency Personnel Processing this, Date, NOTE For renewals and replacements, HSMV REV, and wwwflhsmvgov field.

Feel free to specify the rights and obligations of the parties within the Submit a copy of the registration, Please visit our online renewal, APPLICATION REQUIREMENTS, The form HSMV must be accurately, A Florida driver license number or, Fees There is no charge for a, Note If a second Temporary Parking, CERTIFYING AUTHORITIES, The PhysicianCertifying, and Physician licensed to practice paragraph.

End by reviewing the following sections and preparing them as required: Proof of identity is required when, Check your local phone book, and wwwflhsmvgov.

Step 3: Press the button "Done". The PDF form is available to be transferred. You can easily obtain it to your laptop or send it by email.
Step 4: Have at least two or three copies of the form to avoid all of the possible future troubles.
