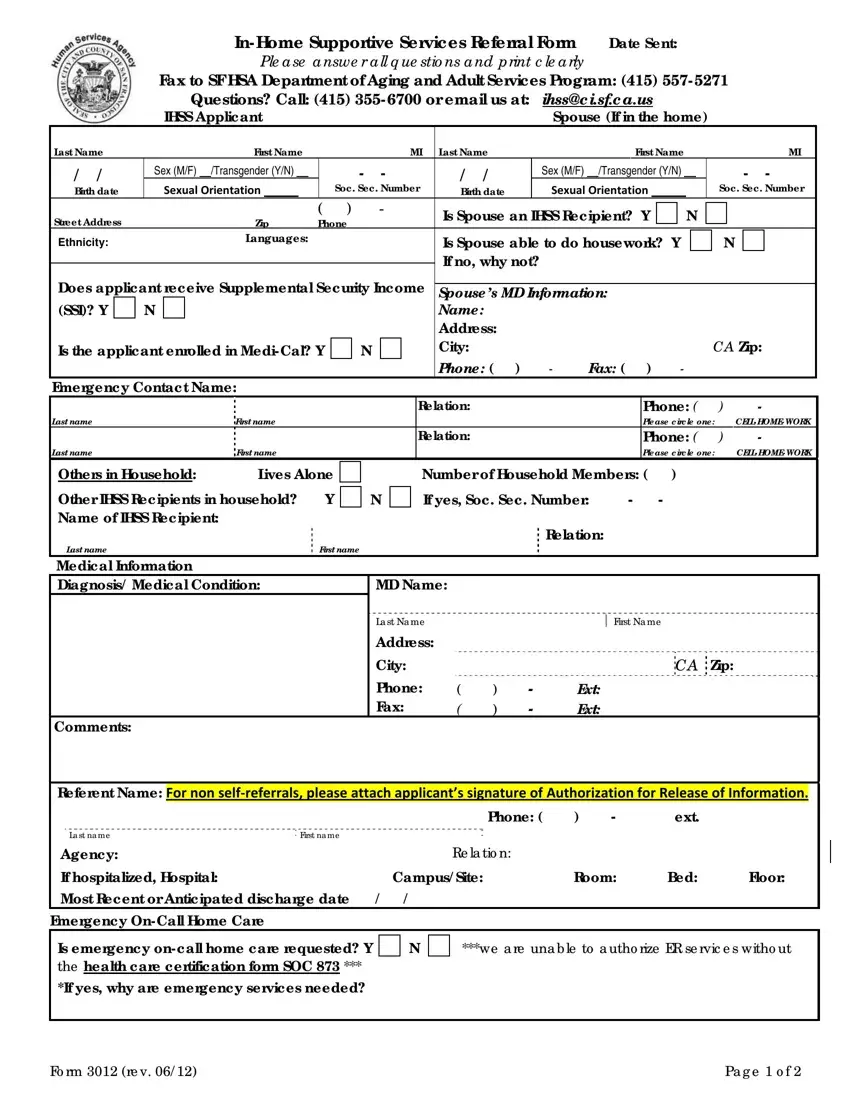
Access to in-home supportive services (IHSS) is a critical component for many individuals seeking assistance with daily living activities, and the IHSS Referral Form plays a pivotal role in connecting applicants with these essential services. This comprehensive document, which must be faxed to the San Francisco Human Services Agency's Department of Aging and Adult Services, requires detailed information about the applicant, any residing spouse, and other household members. It covers a vast array of information, including personal identification, medical conditions, current living situation, and detailed questions regarding the functional ability of the applicant in carrying out activities of daily living. Significantly, the form also probes into the applicant's current level of support, exploring whether emergency on-call home care is needed and if there are any existing services being received or of interest. The importance of providing a complete and accurate referral form cannot be overstated, as it directly influences the applicant's eligibility and the speed at which services can be provided. Moreover, the inclusion of medical information, a signature authorizing the release of information for non-self referrals, and other critical data points ensures a holistic assessment of the applicant's situation, facilitating a tailored response from IHSS. This form represents the first step towards accessing vital in-home support, emphasizing the necessity of clarity and completeness in its submission.
| Question | Answer |
|---|---|
| Form Name | Ihss Referral Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ihss application pdf, ihss recipient application form, ihss orientation, ihss forms |
