


We were developing our PDF editor with the notion of allowing it to be as quick to work with as it can be. That's the reason the procedure of filling in the how to indiana form application healthy plan will be smooth perform all of these steps:
Step 1: Search for the button "Get Form Here" on the following webpage and hit it.
Step 2: Now you will be within the file edit page. You can include, alter, highlight, check, cross, add or delete areas or words.
You'll have to provide the following information in order to fill out the file:
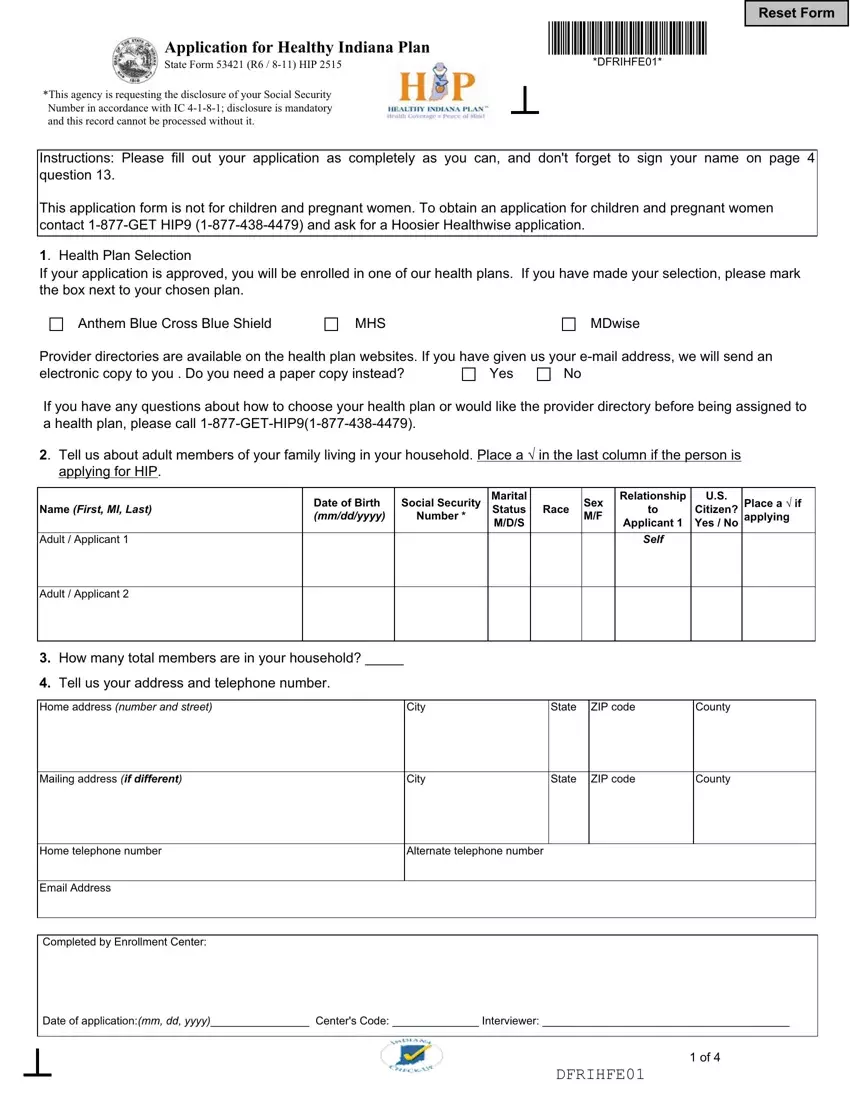
Include the asked particulars in the Mailing address if different, City, State, ZIP code, County, Home telephone number, Alternate telephone number, Email Address, Completed by Enrollment Center, Date of applicationmm dd yyyy, and DFRIHFE segment.
The application will ask for more information with the intention to effortlessly complete the area Child, Child Relation to Applicant, Child, Child Relation to Applicant, Child, Child Relation to Applicant, Child, Child Relation to Applicant, Child Relation to Applicant, Child Relation to Applicant, Child Relation to Applicant, Child Relation to Applicant, Do all of the applicants live in, Does either of the applicants pay, and If yes does the person for whom.
As part of section Applicant Number, Name of person being cared for, How often paid, Amount paid, Name of care provider, Address of provider number and, Complete this section for each, Applicant Number, Document Number, Immigration Status number from, Status Date mmddyy, Country of origin, Date of entry into the US mmddyy, and DFRIHFE, identify the rights and obligations.
Complete the form by taking a look at these particular fields: Applicant has access to health, Covered by health insurance now, Yes No Yes No, Yes No Yes No, Applicant, Applicant, Tell us how much total work, Applicant, Applicant, Start date mmddyy, End date mmddyy, Start date mmddyy, End date mmddyy, Amount of gross pay per period, and Amount of gross pay per period.
Step 3: As soon as you click on the Done button, the finished document is conveniently transferable to any kind of of your devices. Or alternatively, you may send it by means of email.
Step 4: You should generate as many duplicates of your file as you can to stay away from possible troubles.
