It shouldn’t be difficult to fill out risk assessment and screening for telemental health using our PDF editor. Here's how you can rapidly prepare your file.
Step 1: Click the "Get Form Now" button to begin the process.
Step 2: Now you can edit the risk assessment and screening for telemental health. You should use the multifunctional toolbar to add, delete, and alter the content material of the file.
Prepare the risk assessment and screening for telemental health PDF and type in the details for every part:
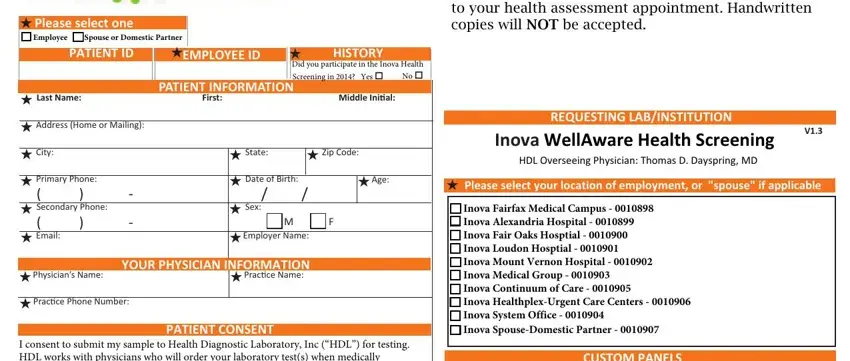
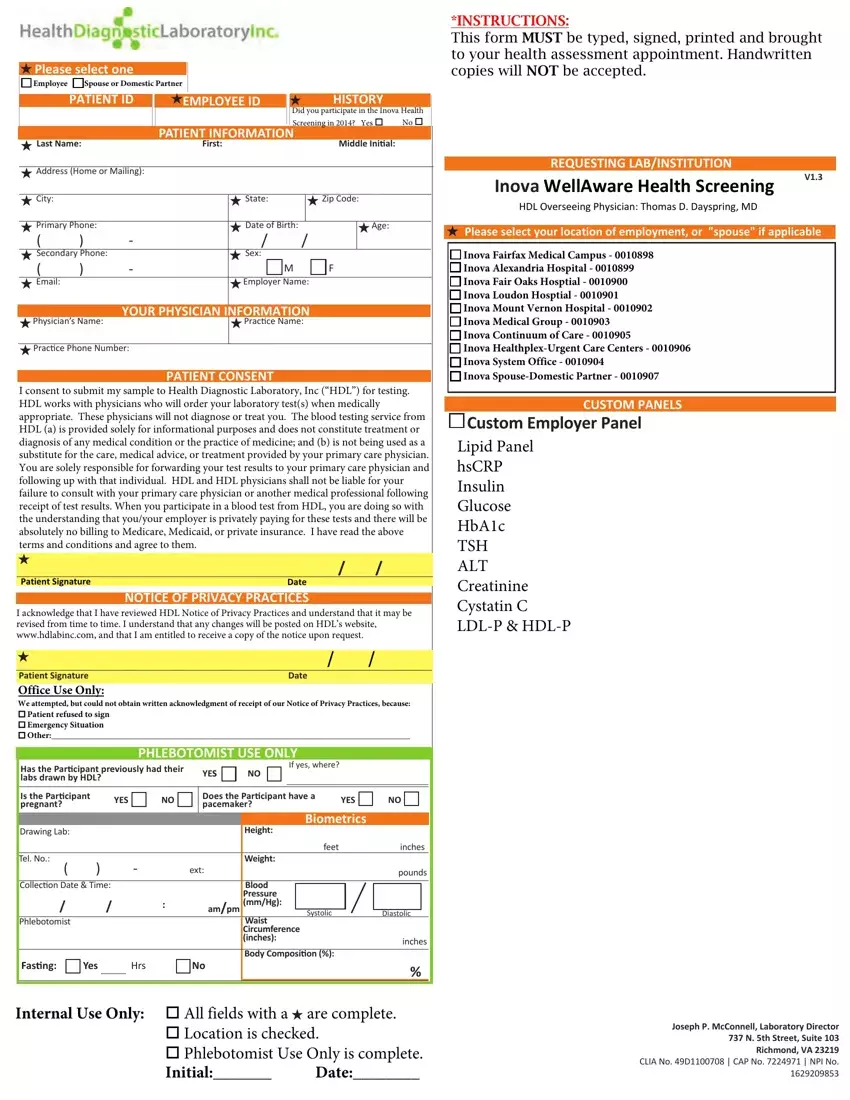
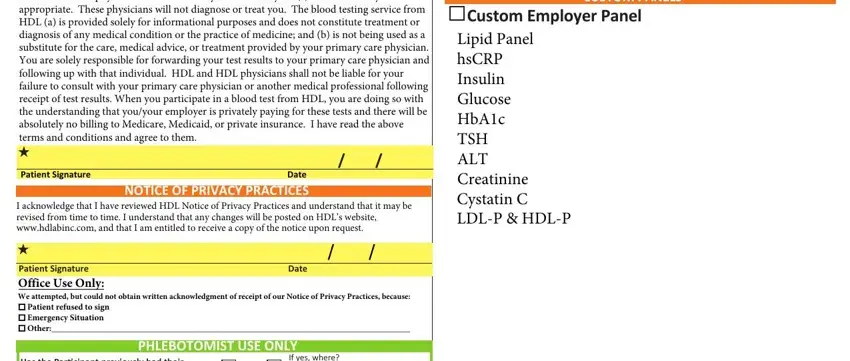
Provide the appropriate data in the field CUSTOM PANELS, Custom Employer Panel, Lipid Panel hsCRP Insulin Glucose, PATIENT CONSENT I consent to, Patient Signature, Date NOTICE OF PRIVACY PRACTICES I, Date, If yes where, and Has the Paricipant previously had.
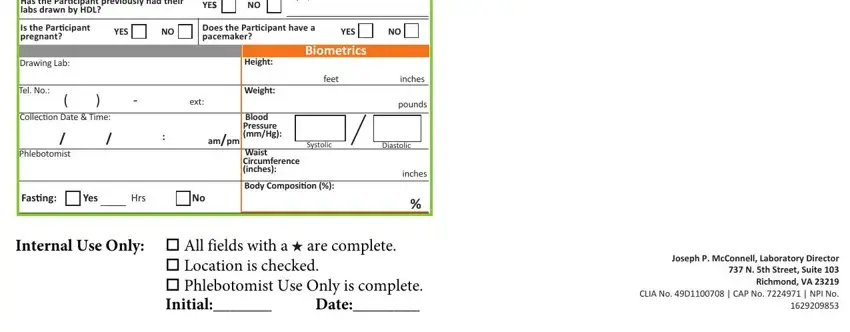
Put together the crucial information in the If yes where, Has the Paricipant previously had, YESS, Is the Paricipant pregnant, YES NO, Does the Paricipant have a, YES NO, Specimen Informaion, Drawing Lab, Tel No, ext, Collecion Date Time, ampm, Phlebotomist, and Height segment.
Step 3: Select the Done button to make certain that your finished document may be exported to any kind of device you want or mailed to an email you specify.
Step 4: It is more convenient to prepare duplicates of the form. There is no doubt that we will not distribute or see your data.
