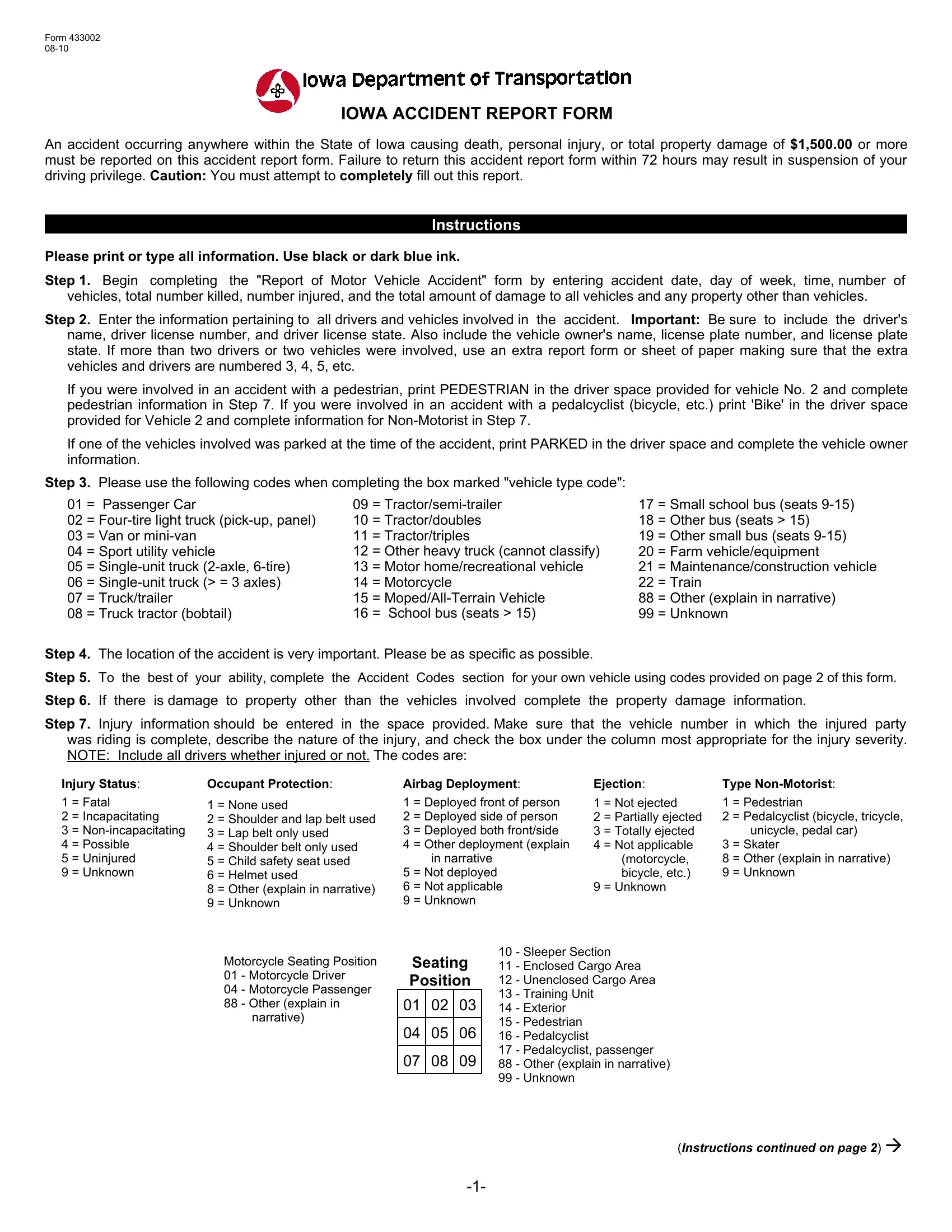


Accurate and timely submission of the Iowa Accident Report Form is crucial, as failure to complete and return it within 72 hours may lead to suspension of driving privileges.
1. Document Accident Details
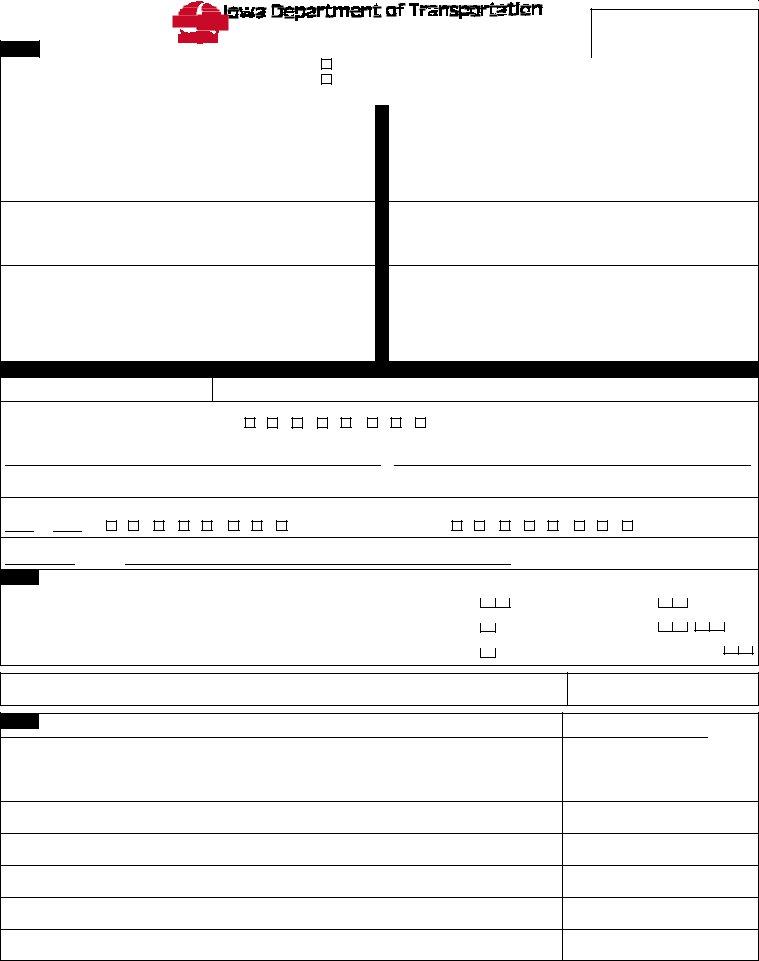
Start by filling out the initial section of the form, which includes the accident date, day of the week, time, and number of vehicles involved. You'll also need to note the total number killed or injured and the total estimated damage to property.
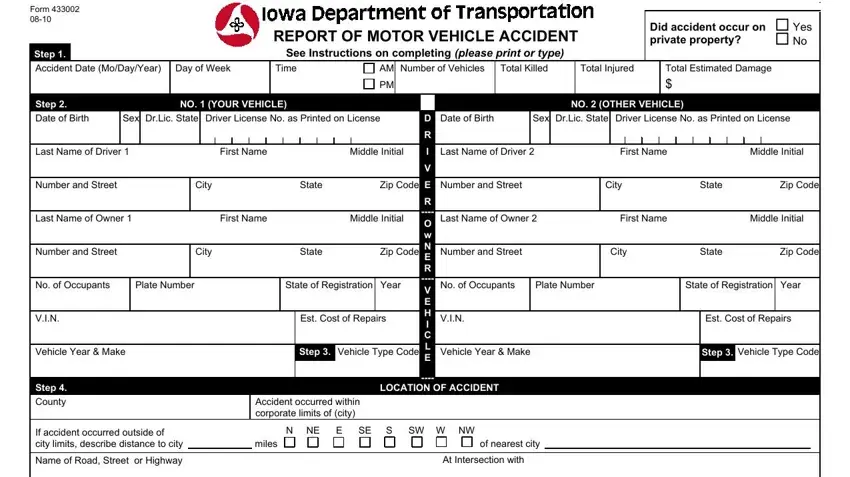
2. Enter Driver and Vehicle Information
Input details for all drivers involved, including names, license numbers, and issuance states. Record the make, model, year, and license plate information for each vehicle.
3. Specify Vehicle Type
For each vehicle involved, select the appropriate vehicle type code from the list provided, which ranges from passenger cars to farm vehicles, ensuring each vehicle type is clearly identified.
4. Describe the Accident Location
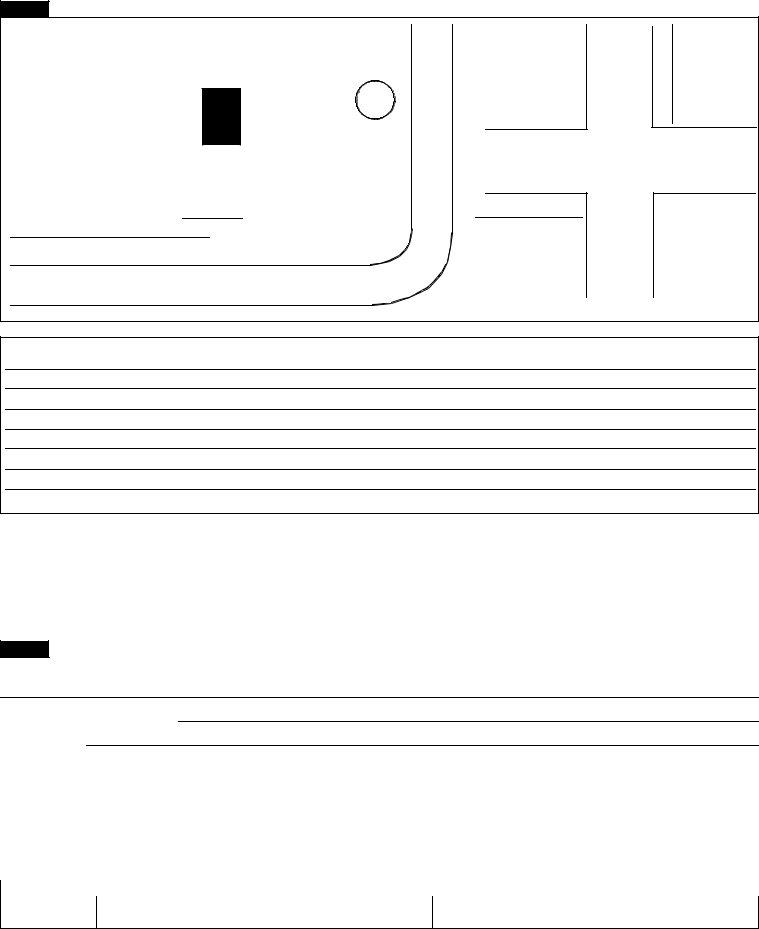
Provide a detailed description of the accident location. Be specific about where the accident occurred, including road names, intersections, and relevant landmarks or features.

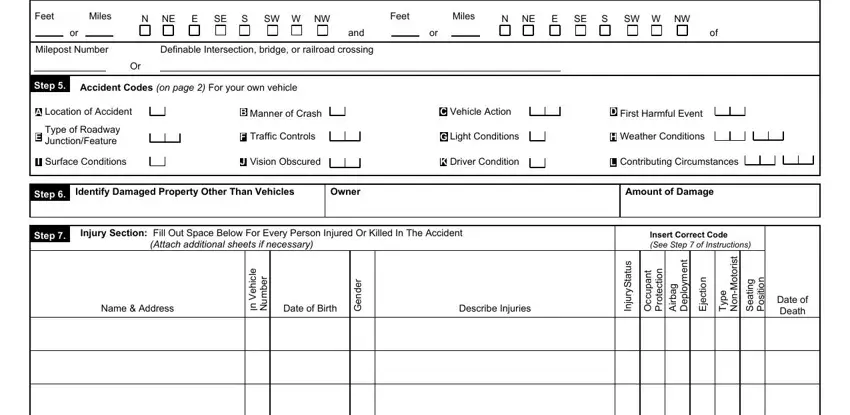
5. Fill in Accident Codes
Using the codes provided on the form, describe your vehicle's involvement in the accident. This includes the type of collision, the nature of any non-collision events, and other specifics outlined by the accident code guidelines.
6. Report Property Damage
If the accident involved damage to property other than vehicles, clearly detail this in the designated section. Include the type of property damaged, the owner's information, and an estimate of the repair costs.
7. Include Injury Information
Document any injuries that occurred as a result of the accident. Specify the vehicle each injured party was in, describe the nature of their injuries, and use the provided codes to indicate the severity of each injury.
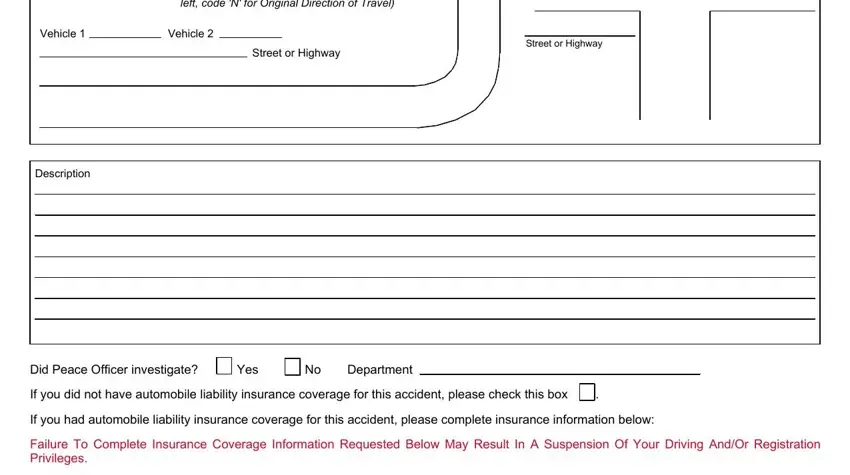
8. Complete the Diagram and Narrative
Draw a diagram of the accident on the provided space and write a detailed narrative describing the events leading up to, during, and after the accident.
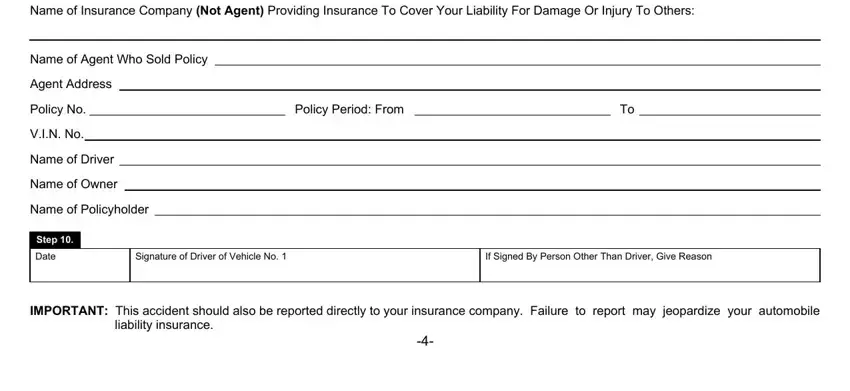
9. Fill Out Insurance Information
Enter comprehensive insurance details for all parties involved. This includes the insurance company name, policy number, and the coverage period.
10. Sign and Review
Review the information for accuracy and completeness after filling out all sections of the form. Sign the form to attest to the truthfulness of the information provided.