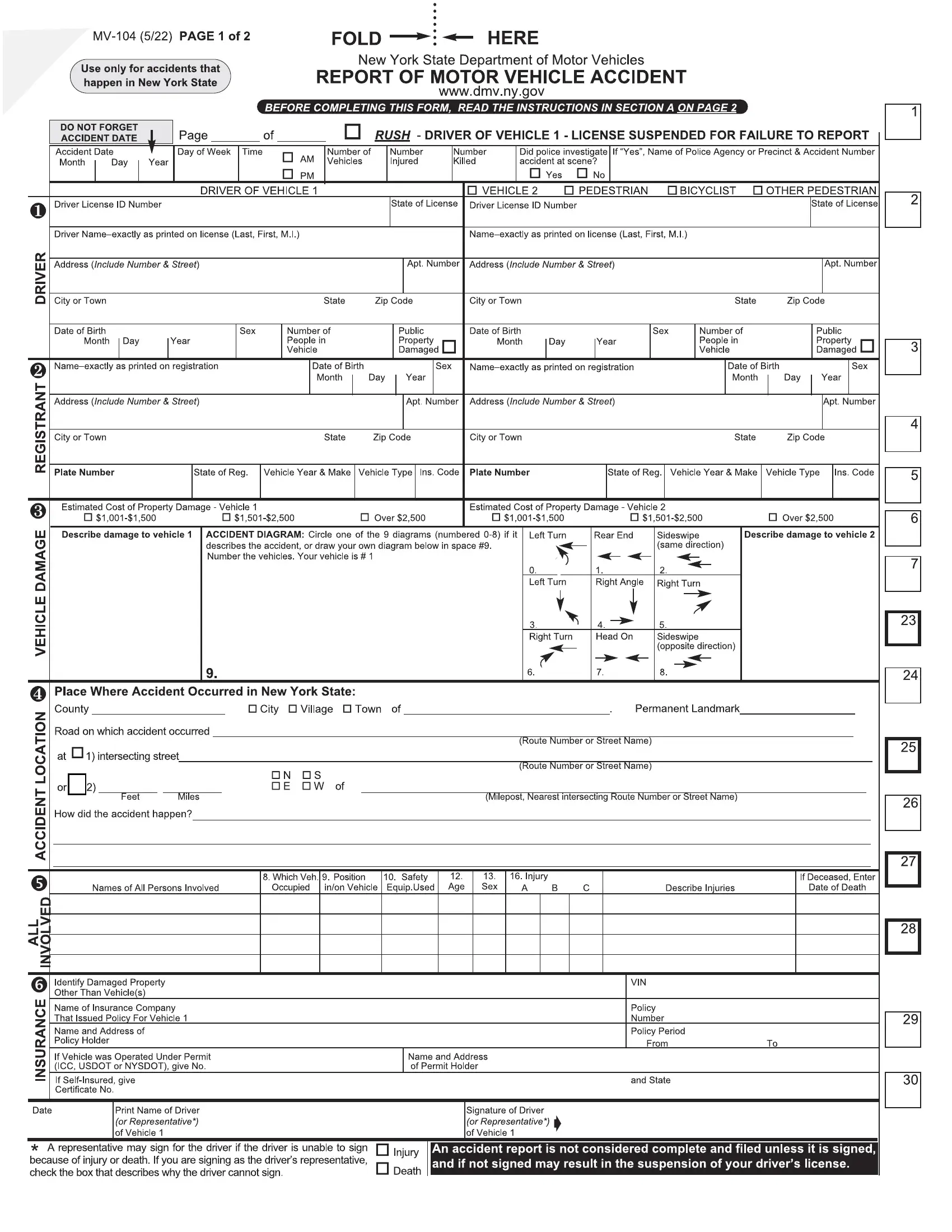
When a motor vehicle accident occurs in New York State, the involved parties must fill out the MV-104 form, a document required by the DMV. This form is an official accident report and plays a key role in the administrative processing of accidents, impacting everything from insurance claims to legal proceedings.
The MV-104 form captures the date, time, location, and description of the accident, along with personal information about the drivers, vehicles involved, and any injuries or fatalities. On the second page, it highlights the significance of reporting accidents that result in personal injury, death, or property damage exceeding $1,000 within ten days, underlining the legal obligations and repercussions of non-compliance. Furthermore, it features instructions for accurately depicting the accident scene and documenting all involved vehicles and pedestrians.
| Question | Answer |
|---|---|
| Form Name | MV 104 Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 104 |
| Avg. time to fill out | 15 min |
| Other names | MV 104 form 7 05, MV104 form, MV 104, MV 104a police accident report |