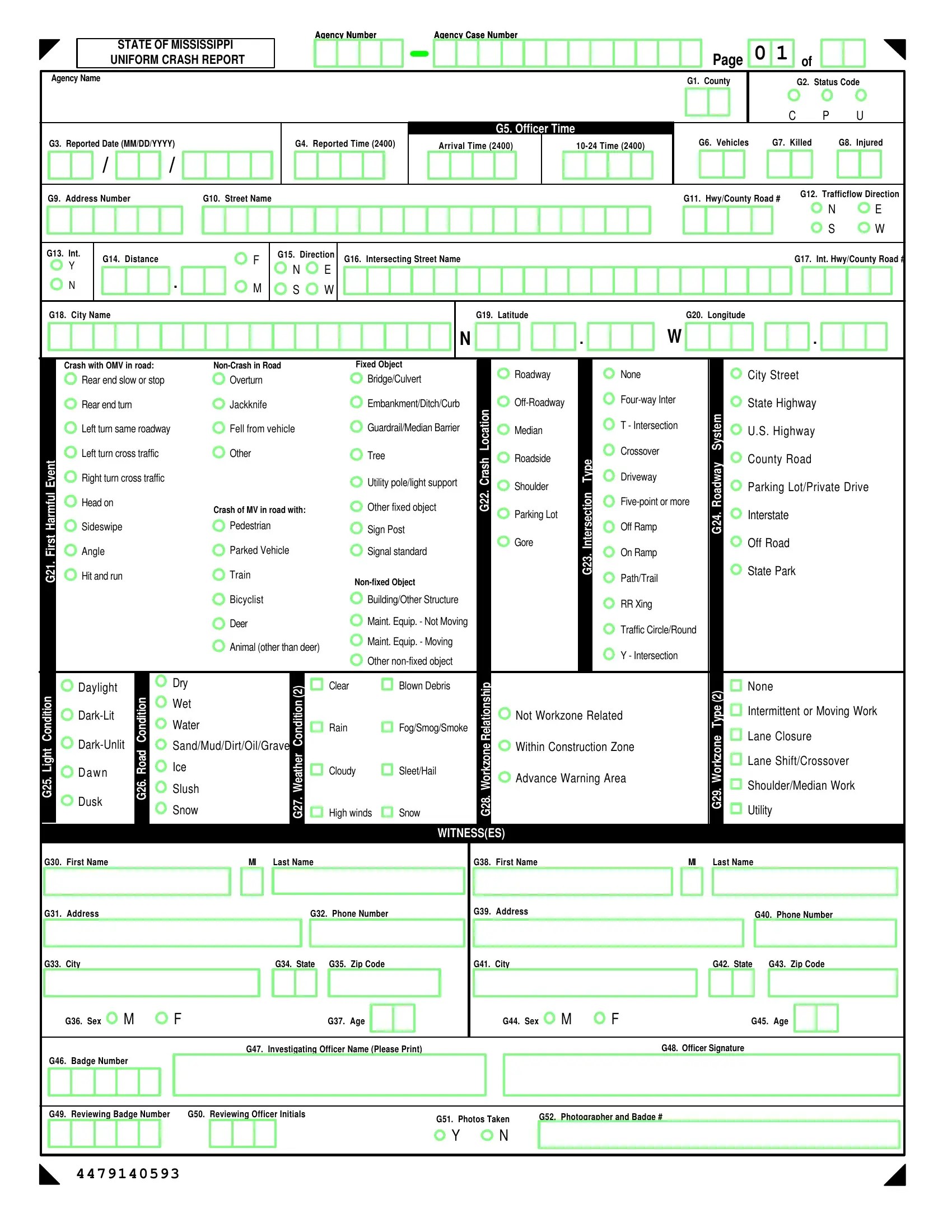
In the realm of road safety and law enforcement, the State of Mississippi Uniform Crash Report plays a pivotal role. Crafted to meticulously document every aspect of road incidents, this form encapsulates critical data ranging from basic identification details like agency and case numbers, to comprehensive descriptors of the accident scene. It encompasses the specifics of the location, capturing county, highway or road numbers, and even geographical coordinates, to offer a clear context. The form details involved vehicles and persons, including drivers, pedestrians, and additional occupants, alongside a narrative and diagram section for a precise depiction of events. Key elements such as the type of accident, whether it involved other moving vehicles, pedestrians, or fixed objects, and the road conditions at the time, are carefully recorded. Witnesses, if any, are also documented, adding layers of verification to the reported facts. Additionally, the report delves into the aftermath in terms of injuries or fatalities, types of safety equipment used, and the deployment status of car airbags, providing a granular view of the incident’s impact. This exhaustive document serves multiple purposes, from aiding law enforcement in investigations to informing policy adjustments for better road safety, making it an indispensable tool in the ongoing effort to safeguard Mississippi’s roadways.
| Question | Answer |
|---|---|
| Form Name | Mississippi Accident Report Form |
| Form Length | 5 pages |
| Fillable fields | 120 |
| Avg. time to fill out | 15 min |
| Other names | Mississippi uniform crash report, Mississippi accident self report form, Mississippi uniform crash report insruction manual 2020, Mississippi highway patrol accident reports |