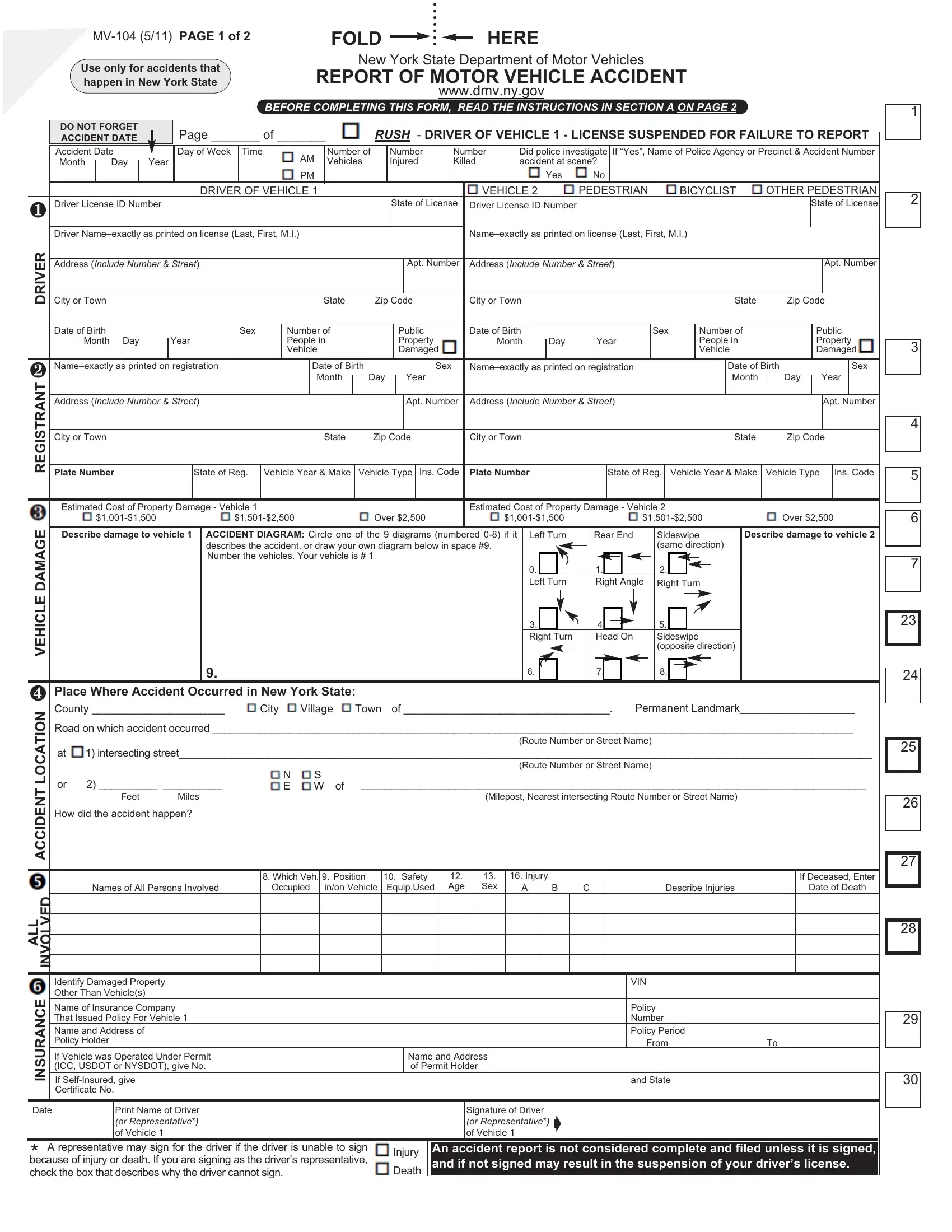
In New York State, residents involved in vehicle accidents causing fatalities, injuries, or property damage exceeding $1,000 must complete and submit the MV-104 form to the New York State Department of Motor Vehicles (DMV). This comprehensive document requests detailed information on the involved parties, the location of the accident, and the circumstances surrounding the event. Besides personal and vehicle information for all parties involved, the form requires an accident diagram, descriptions of vehicle damage, and an assessment of injuries. The accident location is to be specified with both a description and a diagram to offer clear understanding of how the incident occurred. The necessity to report within 10 days of the accident is underlined by the potential legal ramifications of failing to do so, including the classification of such failure as a misdemeanor and the possibility of license and/or registration suspension until the report is filed. Intended to facilitate an objective and comprehensive account of the incident for the DMV records, the MV-104 form plays a critical role in post-accident procedures, emphasizing the importance of accuracy and promptness in its completion and submission.
| Question | Answer |
|---|---|
| Form Name | MV 104 NY Report Accident Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 150 |
| Avg. time to fill out | 12 min |
| Other names | DMV 104, report an accident, NY accident report, NY report accident |