

You can fill out iowa report form accident effectively by using our PDF editor online. The tool is continually updated by our team, acquiring handy functions and turning out to be even more versatile. All it requires is a few simple steps:
Step 1: Click on the "Get Form" button above on this page to open our editor.
Step 2: Using our handy PDF editing tool, you'll be able to do more than just fill out blank form fields. Edit away and make your docs appear great with customized text put in, or modify the file's original input to excellence - all supported by an ability to add stunning images and sign the document off.
In an effort to fill out this document, make sure you type in the information you need in each blank:
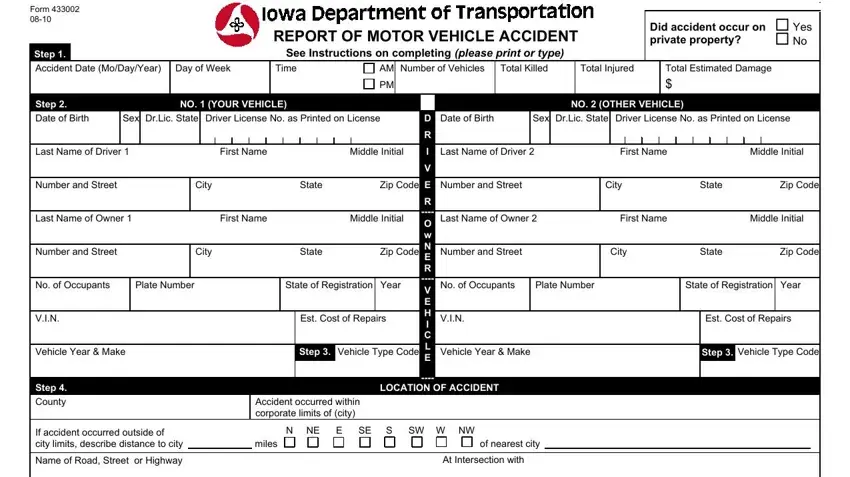
1. Whenever completing the iowa report form accident, make certain to include all important blanks within its relevant part. This will help facilitate the work, enabling your information to be processed fast and appropriately.
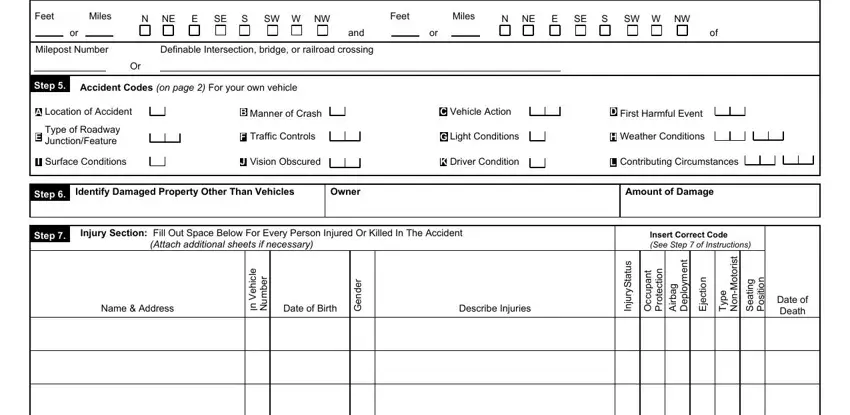
2. Once your current task is complete, take the next step – fill out all of these fields - Note Unless accident occurred at, Feet Miles, N NE, E SE, S SW W NW, Feet Miles, N NE, E SE, S SW W NW, and, Milepost Number, Definable Intersection bridge or, Step, Accident Codes on page For your, and Location of Accident with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. This 3rd segment should be relatively straightforward, Complete reverse side - all these form fields must be filled out here.

It's easy to make a mistake while completing the Complete reverse side, for that reason ensure that you take a second look before you'll finalize the form.
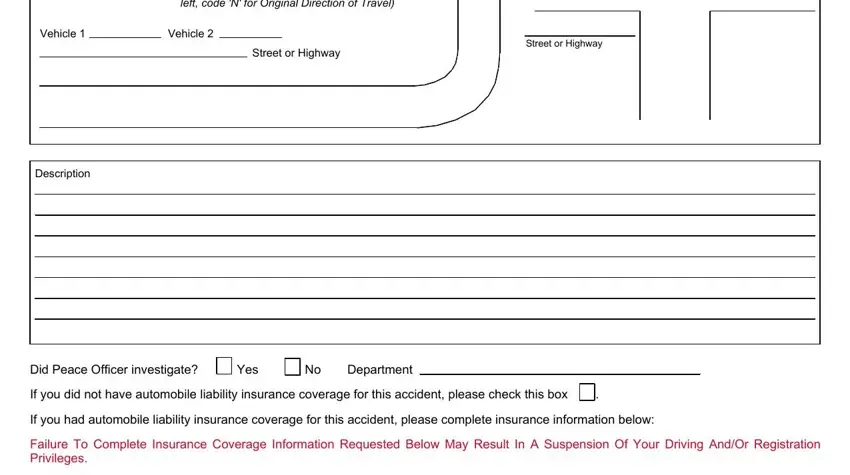
4. The fourth subsection comes next with the next few blank fields to fill out: left code N for Original Direction, Vehicle, Vehicle, Street or Highway, Street or Highway, Description, Did Peace Officer investigate, Yes, No Department, If you did not have automobile, If you had automobile liability, and Failure To Complete Insurance.
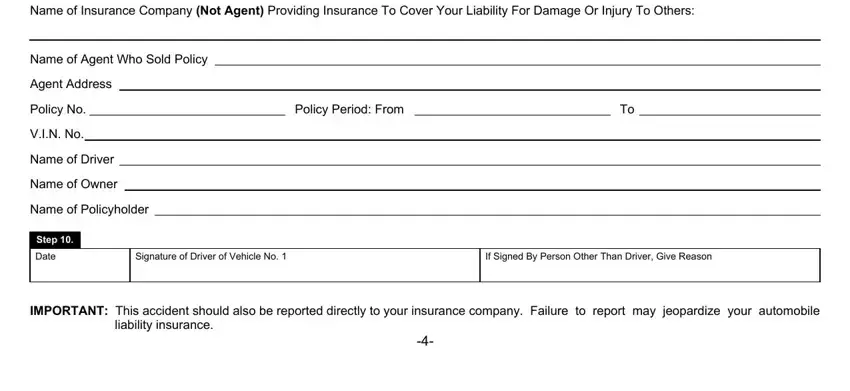
5. The document should be finalized by going through this area. Here you can see an extensive listing of blanks that require correct details in order for your document submission to be faultless: Name of Insurance Company Not, Name of Agent Who Sold Policy, Agent Address, Policy No, VIN No, Name of Driver, Name of Owner, Name of Policyholder, Policy Period From, Step, Date, Signature of Driver of Vehicle No, If Signed By Person Other Than, IMPORTANT This accident should, and liability insurance.
Step 3: Proofread everything you've inserted in the blank fields and click the "Done" button. Join us today and instantly get access to iowa report form accident, all set for downloading. Every last change made is handily preserved , making it possible to edit the pdf at a later point if required. FormsPal is focused on the personal privacy of our users; we ensure that all personal information coming through our system continues to be confidential.