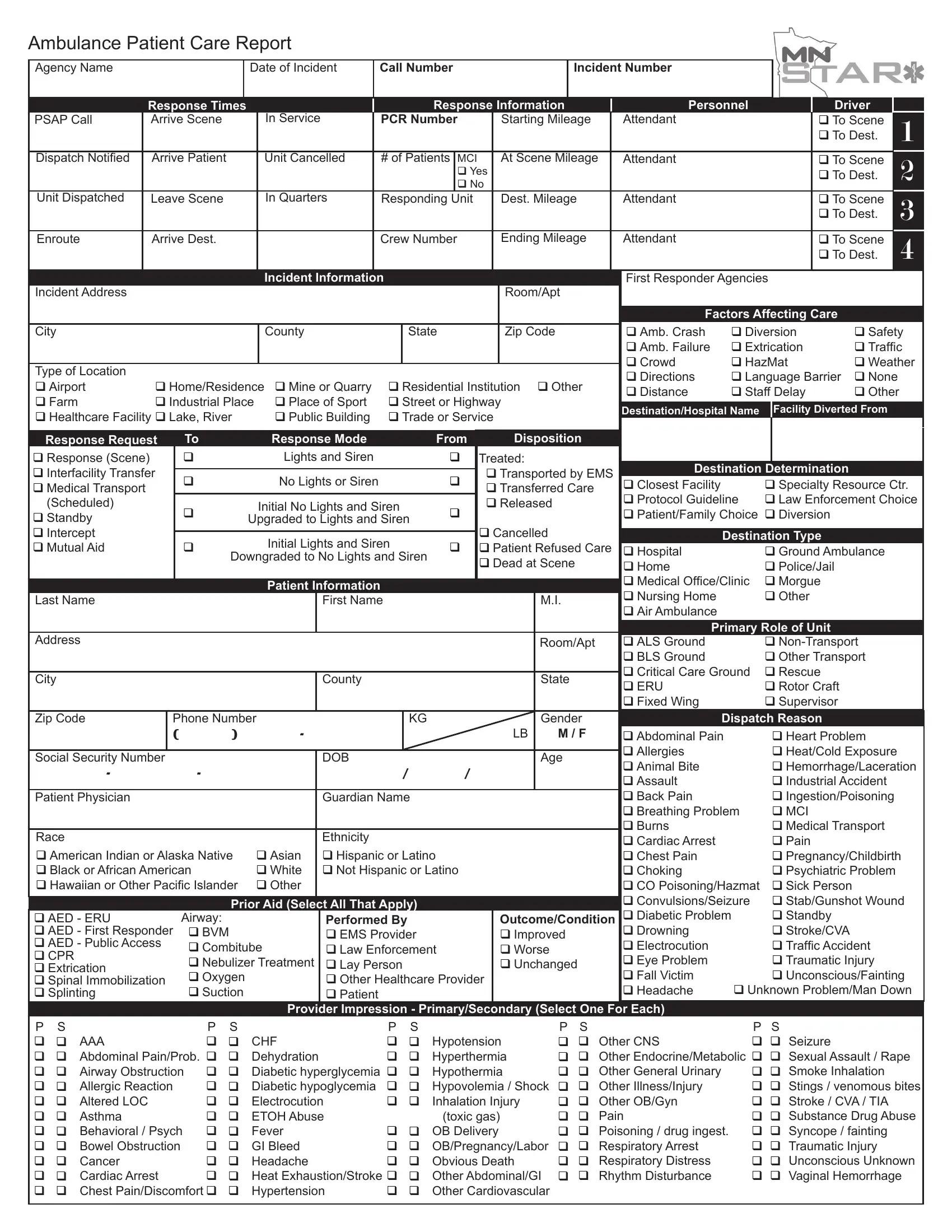
The Irish Ambulance Patient Care Report form is a comprehensive document used by ambulance services to record vital details during emergency response situations. It includes various sections such as agency name, incident number, response times, and personnel involved, ensuring a structured approach to documenting the complexity of care provided. The form captures all aspects of the incident, from the initial dispatch call through to the patient's arrival at the destination, including response information like the number of patients, any mass casualty incidents (MCI), and details on the attending crew. Additionally, it provides space to record critical patient information, medical history, incident specifics, initial assessment, treatments administered, and the eventual patient outcome. This thorough record-keeping aids in continuity of care, facilitates accurate billing, and ensures compliance with regulatory requirements. It also helps in reviewing the response to incidents for quality improvement purposes. The integration of factors affecting care, such as environmental conditions and potential barriers to patient care, alongside detailed records of any pre-existing conditions, medications, and allergies, underscores the form's role in fostering patient-centered care in emergency medical services.
| Question | Answer |
|---|---|
| Form Name | Irish Ambulance Patient Care Report Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | 1099 reporting non reporting chart, patient care report template, printable ambulance report, ambulance patient care report form |
Ambulance Patient Care Report
Agency Name |
|
|
|
|
|
|
|
|
Date of Incident |
|
Call Number |
|
|
|
|
|
Incident Number |
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
Response Times |
|
|
|
|
|
|
|
Response Information |
|
Personnel |
|
|
|
Driver |
|
||||||||||||||||||
PSAP Call |
|
Arrive Scene |
|
|
In Service |
|
PCR Number |
|
|
Starting Mileage |
|
Attendant |
|
|
|
|
To Scene |
|
1 |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To Dest. |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Dispatch Notified |
|
Arrive Patient |
|
|
Unit Cancelled |
|
# of Patients |
MCI |
|
|
At Scene Mileage |
|
Attendant |
|
|
|
|
To Scene |
|
2 |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
|
|
|
|
|
|
|
|
To Dest. |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Unit Dispatched |
|
Leave Scene |
|
|
In Quarters |
|
Responding Unit |
|
|
Dest. Mileage |
|
Attendant |
|
|
|
|
To Scene |
|
3 |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To Dest. |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Enroute |
|
Arrive Dest. |
|
|
|
|
|
Crew Number |
|
|
Ending Mileage |
|
Attendant |
|
|
|
|
To Scene |
|
4 |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To Dest. |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Incident Information |
|
|
|
|
|
|
|
|
|
|
|
|
First Responder Agencies |
|
|
|
||||||
Incident Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Room/Apt |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Factors Affecting Care |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amb. Crash |
Diversion |
Safety |
||||||
City |
|
|
|
|
|
|
|
|
|
|
|
|
County |
|
State |
|
|
Zip Code |
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amb. Failure |
Extrication |
Traffic |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Crowd |
HazMat |
Weather |
||||||
Type of Location |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Directions |
Language Barrier |
None |
|
||||||||
Airport |
Home/Residence |
Mine or Quarry |
Residential Institution Other |
|
|||||||||||||||||||||||||||||||
Distance |
Staff Delay |
Other |
|
||||||||||||||||||||||||||||||||
Farm |
|
|
Industrial Place |
Place of Sport |
Street or Highway |
|
|
|
|
||||||||||||||||||||||||||
Healthcare Facility Lake, River |
|
|
Public Building |
Trade or Service |
|
|
|
Destination/Hospital Name |
|
Facility Diverted From |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Response Request |
|
|
|
To |
|
|
|
|
Response Mode |
|
|
From |
|
|
Disposition |
|
|
|
|
|
|
|
|
|
|||||||||||
Response (Scene) |
|
|
|
|
|
|
|
|
|
Lights and Siren |
|
|
|
Treated: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Interfacility Transfer |
|
|
|
|
|
|
|
No Lights or Siren |
|
|
|
Transported by EMS |
Destination Determination |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
Closest Facility |
|
|
Specialty Resource Ctr. |
||||||||||||||||||||||||
Medical Transport |
|
|
|
|
|
|
|
|
|
|
Transferred Care |
|
|
||||||||||||||||||||||
(Scheduled) |
|
|
|
|
|
|
|
|
|
Initial No Lights and Siren |
|
|
Released |
|
|
|
Protocol Guideline |
|
Law Enforcement Choice |
||||||||||||||||
Standby |
|
|
|
|
|
|
|
Upgraded to Lights and Siren |
|
|
|
|
|
|
|
|
Patient/Family Choice Diversion |
|
|
|
|||||||||||||||
Intercept |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cancelled |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
Initial Lights and Siren |
|
|
|
|
|
|
Destination Type |
|
|
|
|||||||||||||||
Mutual Aid |
|
|
|
|
|
|
|
|
|
|
Patient Refused Care |
Hospital |
|
|
Ground Ambulance |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
Downgraded to No Lights and Siren |
|
|
Dead at Scene |
Home |
|
|
Police/Jail |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical Office/Clinic |
|
Morgue |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nursing Home |
|
|
Other |
|
|
|
|||||||
Last Name |
|
|
|
|
|
|
|
|
|
|
|
First Name |
|
|
|
|
|
M.I. |
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Air Ambulance |
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary Role of Unit |
|
|
|
|||||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Room/Apt |
ALS Ground |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BLS Ground |
|
|
Other Transport |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Critical Care Ground |
|
Rescue |
|
|
|
|||
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
County |
|
|
|
|
|
|
|
State |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ERU |
|
|
Rotor Craft |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fixed Wing |
|
|
Supervisor |
|
|
|
||
Zip Code |
|
Phone Number |
|
|
|
|
KG |
|
|
|
|
|
Gender |
|
Dispatch Reason |
|
|
|
|||||||||||||||||
|
|
|
|
( |
|
|
) |
|
|
|
- |
|
|
|
|
|
|
|
|
LB |
|
M / F |
Abdominal Pain |
|
|
Heart Problem |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Allergies |
|
|
|
Heat/Cold Exposure |
|
|||
Social Security Number |
|
|
|
|
|
|
|
DOB |
|
|
|
|
|
|
|
Age |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Animal Bite |
|
|
|
Hemorrhage/Laceration |
|||||||||||||||||
|
- |
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Assault |
|
|
|
Industrial Accident |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Patient Physician |
|
|
|
|
|
|
|
|
|
|
|
Guardian Name |
|
|
|
|
|
|
|
|
|
Back Pain |
|
|
|
Ingestion/Poisoning |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Breathing Problem |
|
|
MCI |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Burns |
|
|
|
Medical Transport |
|
|||
Race |
|
|
|
|
|
|
|
|
|
|
|
|
|
Ethnicity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cardiac Arrest |
|
|
|
Pain |
|
|
|
||||
American Indian or Alaska Native |
Asian |
Hispanic or Latino |
|
|
|
|
|
|
|
Chest Pain |
|
|
|
Pregnancy/Childbirth |
|||||||||||||||||||||
Black or African American |
|
|
White |
Not Hispanic or Latino |
|
|
|
|
|
|
|
Choking |
|
|
|
Psychiatric Problem |
|
||||||||||||||||||
Hawaiian or Other Pacific Islander |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
CO Poisoning/Hazmat |
|
Sick Person |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Convulsions/Seizure |
|
|
Stab/Gunshot Wound |
|||||||||
|
|
|
|
|
|
|
|
|
Prior Aid (Select All That Apply) |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
AED - ERU |
|
|
|
|
Airway: |
|
|
|
Performed By |
|
|
|
|
Outcome/Condition |
Diabetic Problem |
|
|
Standby |
|
|
|
||||||||||||||
AED - First Responder |
|
BVM |
|
|
|
EMS Provider |
|
|
|
|
Improved |
Drowning |
|
|
|
Stroke/CVA |
|
|
|
||||||||||||||||
AED - Public Access |
|
Combitube |
|
Law Enforcement |
|
|
Worse |
|
|
|
Electrocution |
|
|
|
Traffic Accident |
|
|||||||||||||||||||
CPR |
|
|
|
|
|
|
|
Nebulizer Treatment |
Lay Person |
|
|
|
|
Unchanged |
Eye Problem |
|
|
|
Traumatic Injury |
|
|||||||||||||||
Extrication |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Spinal Immobilization |
|
Oxygen |
|
|
|
Other Healthcare Provider |
|
|
|
|
|
Fall Victim |
|
|
|
Unconscious/Fainting |
|||||||||||||||||||
Splinting |
|
|
|
|
|
Suction |
|
|
|
Patient |
|
|
|
|
|
|
|
|
|
|
|
Headache |
Unknown Problem/Man Down |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Provider Impression - Primary/Secondary (Select One For Each) |
|
|
|
|
|
|
|
|
||||||||||||||
P S |
|
|
|
|
|
|
|
|
P S |
|
|
|
|
|
P S |
|
|
|
|
|
|
P S |
|
|
P |
|
S |
|
|
|
|||||
|
AAA |
|
|
|
|
|
|
|
CHF |
|
Hypotension |
Other CNS |
|
Seizure |
|
|
|
||||||||||||||||||
|
Abdominal Pain/Prob. |
Dehydration |
|
Hyperthermia |
Other Endocrine/Metabolic Sexual Assault / Rape |
||||||||||||||||||||||||||||||
|
Airway Obstruction |
|
|
Diabetic hyperglycemia |
Hypothermia |
Other General Urinary |
|
Smoke Inhalation |
|
||||||||||||||||||||||||||
|
Allergic Reaction |
|
|
|
Diabetic hypoglycemia |
|
Hypovolemia / Shock |
Other Illness/Injury |
|
Stings / venomous bites |
|||||||||||||||||||||||||
|
Altered LOC |
|
|
|
|
|
|
|
Electrocution |
|
Inhalation Injury |
Other OB/Gyn |
|
Stroke / CVA / TIA |
|
||||||||||||||||||||
|
Asthma |
|
|
|
|
|
|
|
ETOH Abuse |
|
|
(toxic gas) |
Pain |
|
Substance Drug Abuse |
||||||||||||||||||||
|
Behavioral / Psych |
|
|
Fever |
|
OB Delivery |
Poisoning / drug ingest. |
Syncope / fainting |
|
||||||||||||||||||||||||||
|
Bowel Obstruction |
|
|
|
GI Bleed |
|
OB/Pregnancy/Labor |
Respiratory Arrest |
|
Traumatic Injury |
|
||||||||||||||||||||||||
|
Cancer |
|
|
|
|
|
|
|
Headache |
|
Obvious Death |
Respiratory Distress |
|
Unconscious Unknown |
|||||||||||||||||||||
|
Cardiac Arrest |
|
|
|
Heat Exhaustion/Stroke |
Other Abdominal/GI |
Rhythm Disturbance |
|
Vaginal Hemorrhage |
||||||||||||||||||||||||||
|
Chest Pain/Discomfort |
Hypertension |
|
Other Cardiovascular |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|