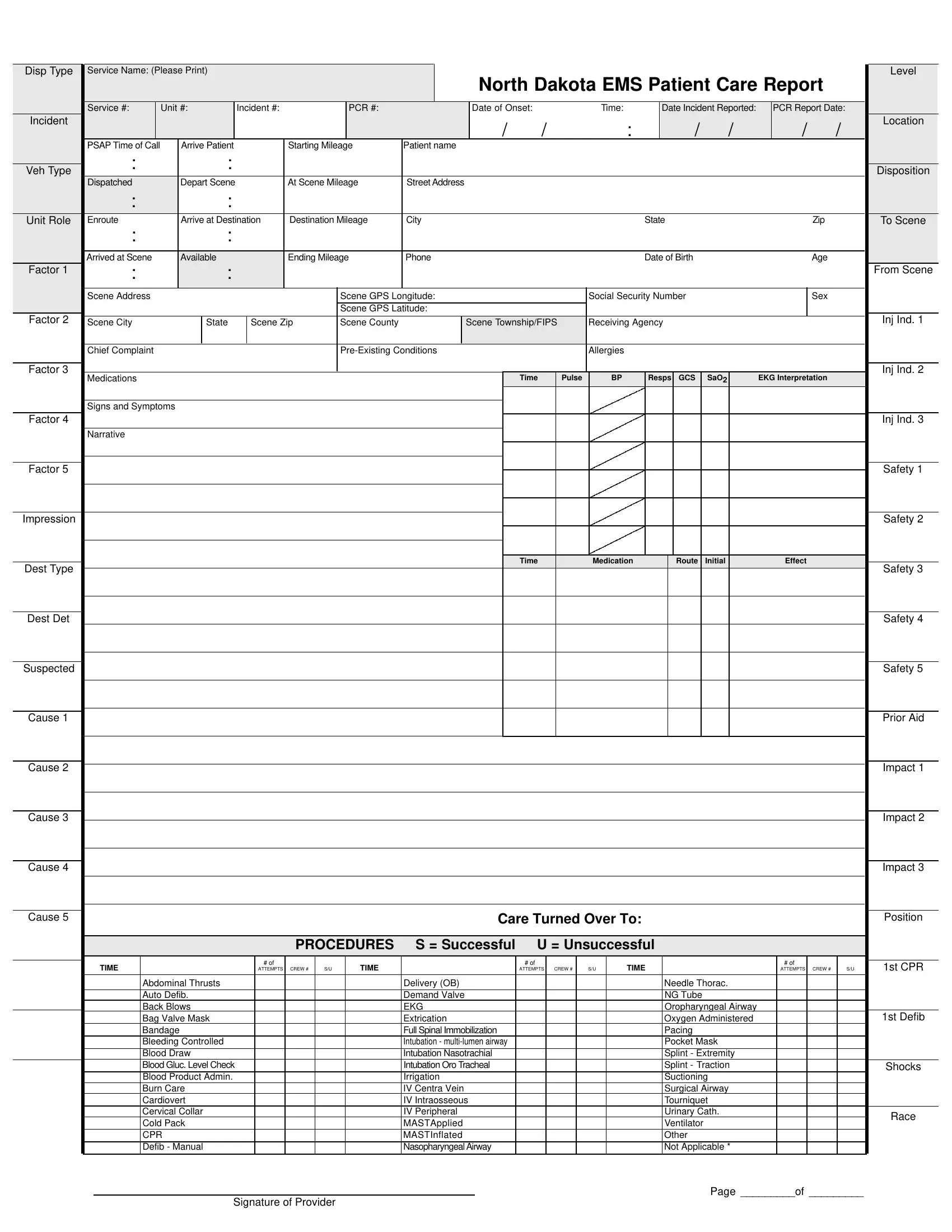
In the realm of emergency medical services (EMS) in North Dakota, the EMS Patient Care Report form represents a crucial document bridging clinical care and administrative requirements. This comprehensive form meticulously records everything from the initial dispatch of EMS services—detailing the service name, level, and unit numbers—to the nuanced data of the patient's experience and treatment during the EMS encounter. It captures key timestamps such as the date and time of the incident, arrival at the scene, and patient departure, alongside logistical information like vehicle type and mileage. The patient's demographic details, including name, date of birth, contact information, and medical identifiers like Social Security Number and health conditions, are systematically logged. Furthermore, it encompasses the medical assessment and interventions performed, categorized by the nature and successfulness of procedures, medication administration specifics, and patient outcomes before handing over to a receiving agency or hospital. In addition to clinical notes, the form also addresses billing information by noting insurance details and capturing both acknowledgment of the receipt of services and, if applicable, refusal of service, ensuring legal and financial clarity. The North Dakota EMS Patient Care Report form, thereby, stands as a critical record, ensuring accurate documentation of pre-hospital care, guiding billing processes, and providing a legal record of the care provided.
| Question | Answer |
|---|---|
| Form Name | North Dakota Ems Patient Care Report Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | emt pcr narrative examples, patient care report narrative examples, ems narrative report template, ems report example |
Disp Type |
Service Name: (Please Print) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Level |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
North Dakota EMS Patient Care Report |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Service #: |
|
Unit #: |
Incident #: |
|
|
|
PCR #: |
|
|
|
Date of Onset: |
|
|
Time: |
|
|
Date Incident Reported: |
|
PCR Report Date: |
|
||||||||||||||||||
Incident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
: |
|
/ |
|
/ |
|
/ |
|
/ |
Location |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
PSAP Time of Call |
|
Arrive Patient |
|
|
|
Starting Mileage |
Patient name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Veh Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Disposition |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Dispatched |
|
Depart Scene |
|
|
|
At Scene Mileage |
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unit Role |
Enroute |
|
Arrive at Destination |
Destination Mileage |
City |
|
|
|
|
|
|
|
State |
|
|
|
|
|
Zip |
|
|
To Scene |
|||||||||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Arrived at Scene |
|
Available |
|
|
|
Ending Mileage |
Phone |
|
|
|
|
|
|
|
Date of Birth |
|
|
|
|
|
Age |
|
|
|
||||||||||||||
Factor 1 |
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From Scene |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scene Address |
|
|
|
|
|
|
|
|
Scene GPS Longitude: |
|
|
|
|
Social Security Number |
|
|
|
|
|
Sex |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Scene GPS Latitude: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Factor 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 1 |
Scene City |
|
|
State |
|
Scene Zip |
|
Scene County |
|
|
Scene Township/FIPS |
Receiving Agency |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chief Complaint |
|
|
|
|
|
|
|
|
|
|
|
|
Allergies |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Factor 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 2 |
|
Medications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
Pulse |
|
BP |
|
Resps |
GCS |
|
SaO2 |
|
EKG Interpretation |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signs and Symptoms |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Factor 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Narrative |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Factor 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impression |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
|
|
Medication |
|
|
|
Route |
|
Initial |
|
|
|
Effect |
|
|
|
||||
Dest Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 3 |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dest Det |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suspected |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Prior Aid |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Care Turned Over To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Position |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROCEDURES |
S = Successful |
U = Unsuccessful |
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
1st CPR |
|||||
|
|
|
|
|
|
|
|
ATTEMPTS |
CREW # |
S/U |
|
|
|
|
|
|
ATTEMPTS |
|
CREW # |
|
S/U |
|
|
|
|
|
|
|
|
ATTEMPTS |
CREW # |
|
S/U |
||||||
|
|
Abdominal Thrusts |
|
|
|
|
|
|
|
Delivery (OB) |
|
|
|
|
|
|
|
|
|
Needle Thorac. |
|
|
|
|
|
|
|
||||||||||||
|
|
Auto Defib. |
|
|
|
|
|
|
|
Demand Valve |
|
|
|
|
|
|
|
|
|
NG Tube |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Back Blows |
|
|
|
|
|
|
|
EKG |
|
|
|
|
|
|
|
|
|
Oropharyngeal Airway |
|
|
|
|
|
|
|
||||||||||||
|
|
Bag Valve Mask |
|
|
|
|
|
|
|
Extrication |
|
|
|
|
|
|
|
|
|
Oxygen Administered |
|
|
|
|
|
|
1st Defib |
||||||||||||
|
|
Bandage |
|
|
|
|
|
|
|
Full Spinal Immobilization |
|
|
|
|
|
|
|
|
|
Pacing |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Bleeding Controlled |
|
|
|
|
|
|
|
Intubation - |
|
|
|
|
|
|
|
|
|
Pocket Mask |
|
|
|
|
|
|
|
||||||||||||
|
|
Blood Draw |
|
|
|
|
|
|
|
Intubation Nasotrachial |
|
|
|
|
|
|
|
|
|
Splint - Extremity |
|
|
|
|
|
|
|
||||||||||||
|
|
Blood Gluc. Level Check |
|
|
|
|
|
|
|
Intubation Oro Tracheal |
|
|
|
|
|
|
|
|
|
Splint - Traction |
|
|
|
|
|
|
Shocks |
||||||||||||
|
|
Blood Product Admin. |
|
|
|
|
|
|
|
Irrigation |
|
|
|
|
|
|
|
|
|
Suctioning |
|
|
|
|
|
|
|
||||||||||||
|
|
Burn Care |
|
|
|
|
|
|
|
IV Centra Vein |
|
|
|
|
|
|
|
|
|
Surgical Airway |
|
|
|
|
|
|
|
||||||||||||
|
|
Cardiovert |
|
|
|
|
|
|
|
IV Intraosseous |
|
|
|
|
|
|
|
|
|
Tourniquet |
|
|
|
|
|
|
|
||||||||||||
|
|
Cervical Collar |
|
|
|
|
|
|
|
IV Peripheral |
|
|
|
|
|
|
|
|
|
Urinary Cath. |
|
|
|
|
|
|
Race |
||||||||||||
|
|
Cold Pack |
|
|
|
|
|
|
|
MASTApplied |
|
|
|
|
|
|
|
|
|
Ventilator |
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
CPR |
|
|
|
|
|
|
|
MASTInflated |
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Defib - Manual |
|
|
|
|
|
|
|
Nasopharyngeal Airway |
|
|
|
|
|
|
|
|
|
Not Applicable * |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page _________of _________
Signature of Provider