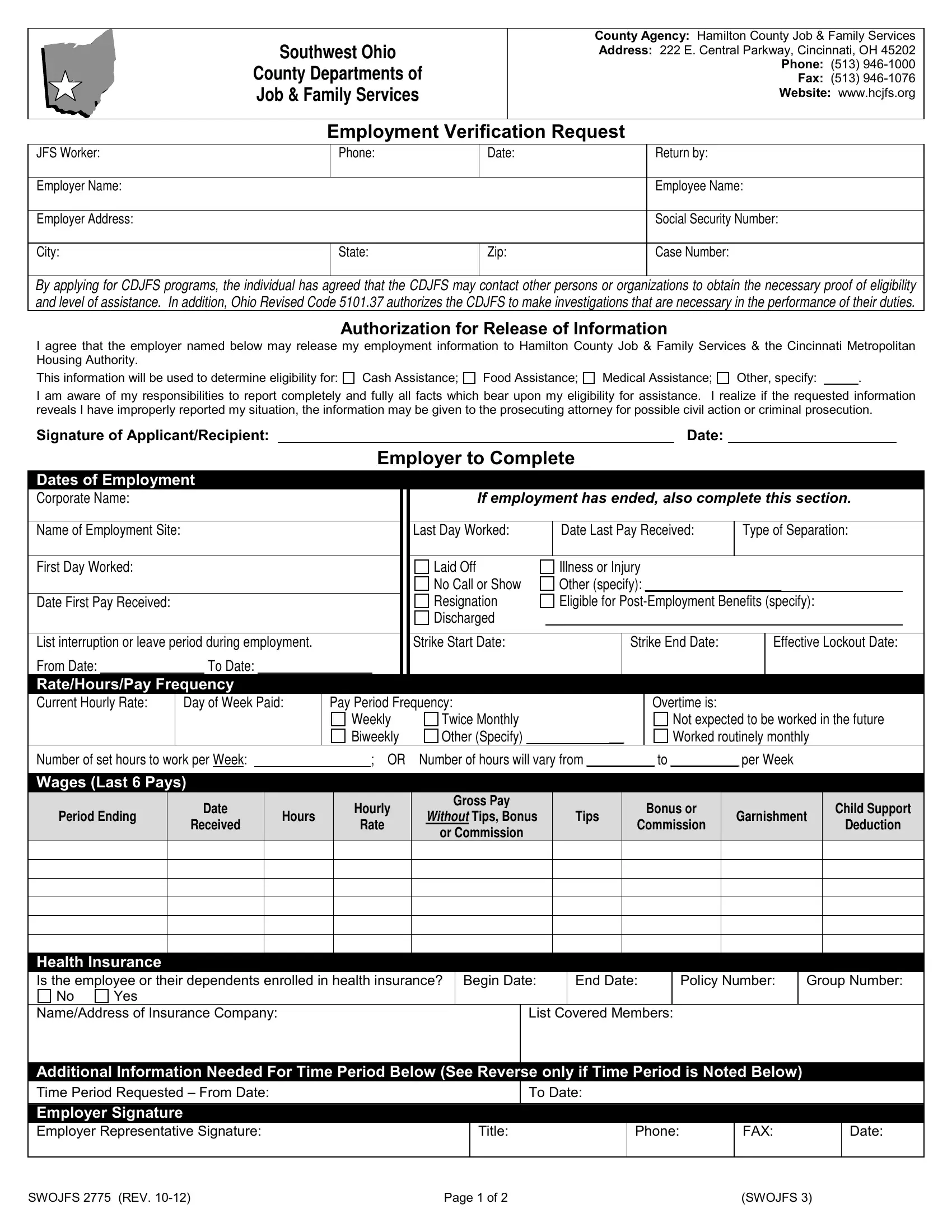
In the realm of public assistance and employment verification within Hamilton County, Ohio, the Job and Family Services Hamilton Ohio form serves as a critical document facilitating communication between employers and the Southwest Ohio County Departments of Job & Family Services. Located at 222 E. Central Parkway in Cincinnati, this agency requires the completion of this form to verify employment details crucial for determining eligibility for various assistance programs such as Cash Assistance, Food Assistance, Medical Assistance, among others. The form, detailed in its requirements, mandates the employer to furnish information regarding the employee's dates of employment, wages, potential benefits, and the reason for separation if applicable, underscoring the comprehensive nature of Ohio's approach to verifying eligibility and ensuring aid reaches those genuinely in need. It emphasizes the legal framework governing such inquiries, including the agreement of applicants to permit the investigation into their circumstances as mandated by Ohio Revised Code 5101.37, and the potential for criminal prosecution should misinformation be revealed. This document underscores the interconnectedness of public assistance programs, employers, and the legal obligations of individuals seeking aid, highlighting the thorough processes in place to maintain integrity and fairness in the distribution of public resources.
| Question | Answer |
|---|---|
| Form Name | Job And Family Services Hamilton Ohio Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | job and family services hamilton ohio, job and family services employment verification form, hamilton county jfs forms, ohio employment verification form |