
When you want to fill out kaiser group enrollment form, you won't have to install any programs - just make use of our PDF tool. Our editor is continually developing to provide the best user experience achievable, and that's due to our commitment to constant improvement and listening closely to user opinions. Here's what you'll need to do to begin:
Step 1: Just press the "Get Form Button" in the top section of this site to open our pdf file editing tool. There you'll find everything that is required to fill out your file.
Step 2: This tool will let you modify your PDF file in many different ways. Improve it with personalized text, correct what's already in the PDF, and add a signature - all within the reach of several clicks!
When it comes to blanks of this specific document, here is what you should consider:
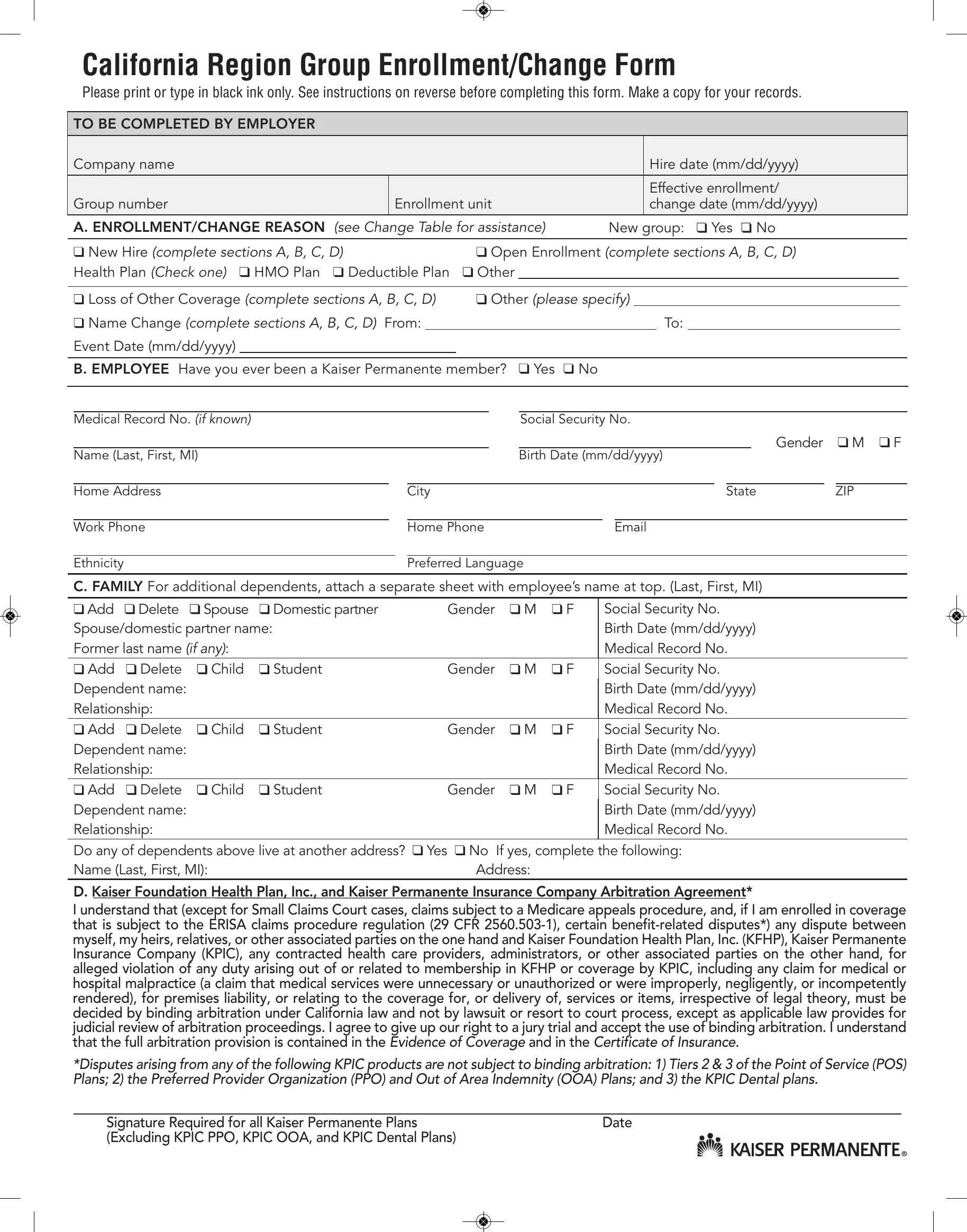
1. To start with, once completing the kaiser group enrollment form, start in the area that has the next blanks:

2. Just after the prior part is filled out, go on to type in the relevant details in all these: C FAMILY For additional dependents, Add, Delete, Spouse, Domestic partner, Gender, Spousedomestic partner name Former, Add, Delete, Child, Student, Gender, Dependent name Relationship, Add, and Delete.
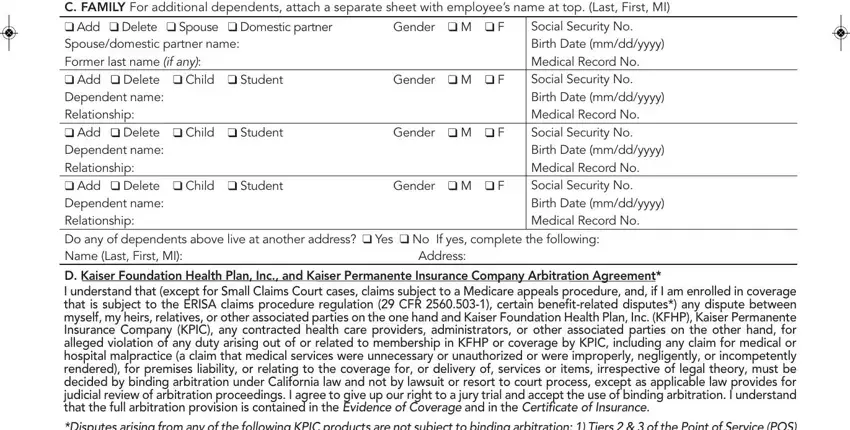
It's easy to make a mistake when filling in your Domestic partner, for that reason be sure to reread it before you decide to submit it.
3. This third step is hassle-free - fill out all the empty fields in Dependent name Relationship Do any, Signature Required for all Kaiser, and Date to complete this process.

Step 3: Make certain the information is right and simply click "Done" to conclude the process. Download the kaiser group enrollment form after you subscribe to a free trial. Easily access the pdf file in your FormsPal account, together with any modifications and adjustments being conveniently synced! FormsPal guarantees safe form editing devoid of personal information recording or sharing. Rest assured that your information is in good hands with us!