
Dealing with PDF documents online is super easy with our PDF tool. You can fill in patient assistance application for vivitrol here without trouble. To maintain our tool on the cutting edge of efficiency, we work to integrate user-driven features and enhancements on a regular basis. We're always grateful for any suggestions - join us in revampimg how we work with PDF files. This is what you'd need to do to start:
Step 1: Open the PDF inside our tool by clicking the "Get Form Button" at the top of this page.
Step 2: As soon as you access the PDF editor, you'll notice the document ready to be filled out. In addition to filling out different blanks, you could also do several other actions with the file, namely adding your own textual content, modifying the original text, adding illustrations or photos, affixing your signature to the form, and much more.
As for the blank fields of this precise PDF, here's what you need to know:
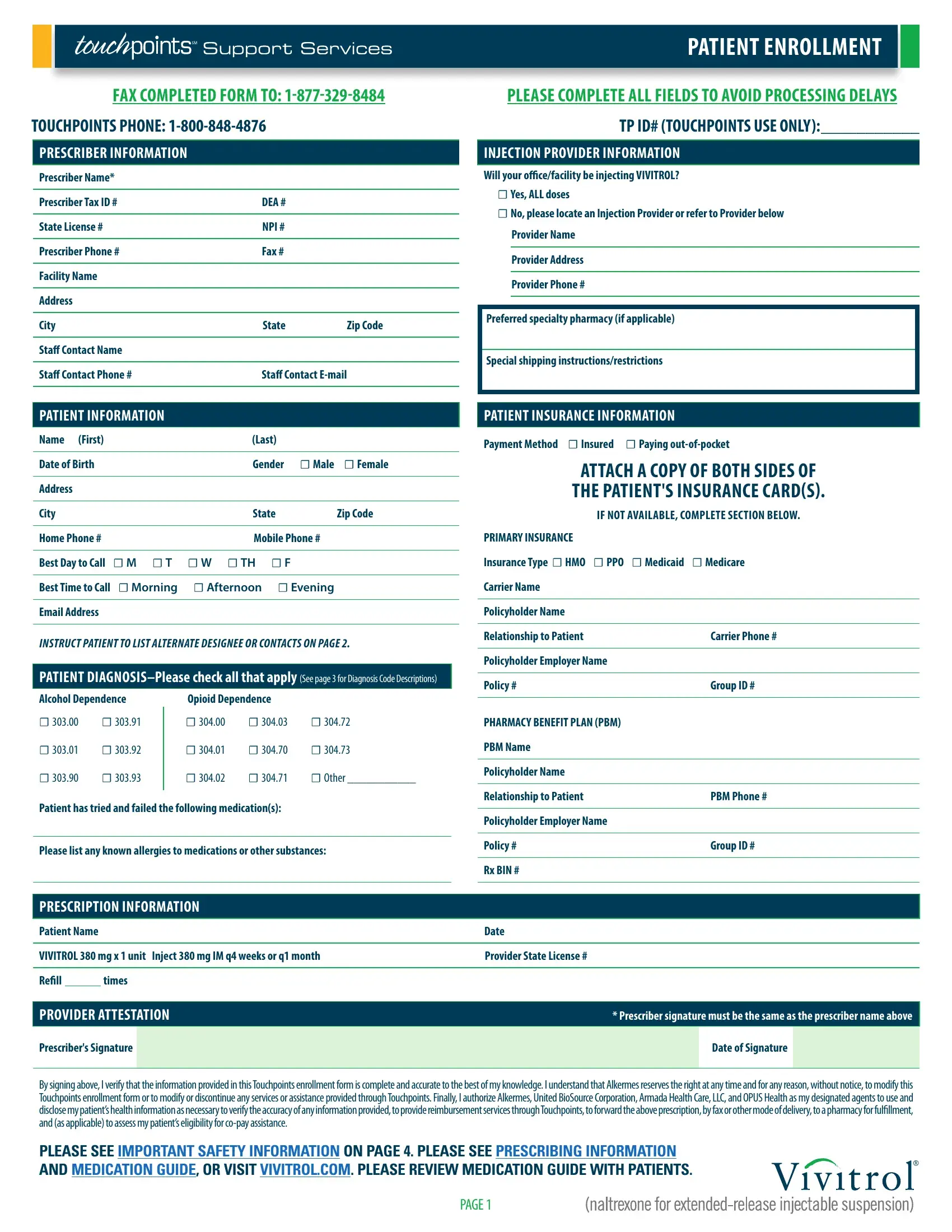
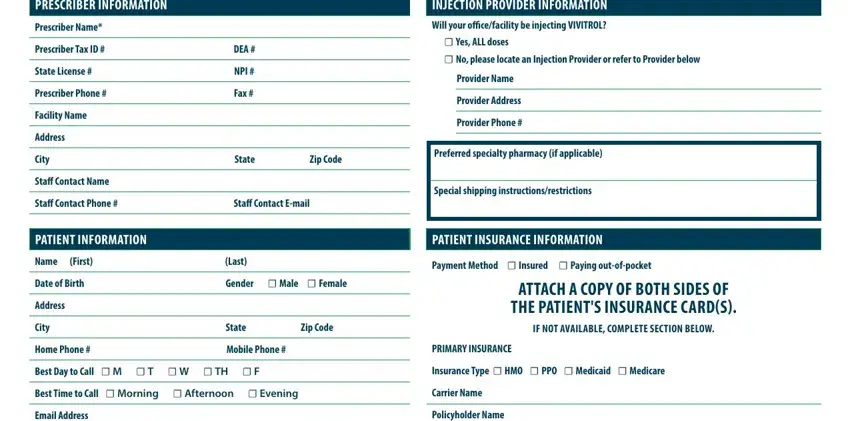
1. Fill out the patient assistance application for vivitrol with a selection of major fields. Get all the necessary information and ensure nothing is omitted!
2. Immediately after the first part is done, go on to type in the relevant details in all these: Email Address, Policyholder Name, INSTRUCT PATIENT TO LIST ALTERNATE, PATIENT DIAGNOSISPlease check all, Alcohol Dependence, Opioid Dependence, Relationship to Patient Carrier, Policyholder Employer Name, Policy Group ID, PHARMACY BENEFIT PLAN PBM, PBM Name, Other, Policyholder Name, Patient has tried and failed the, and Please list any known allergies to.
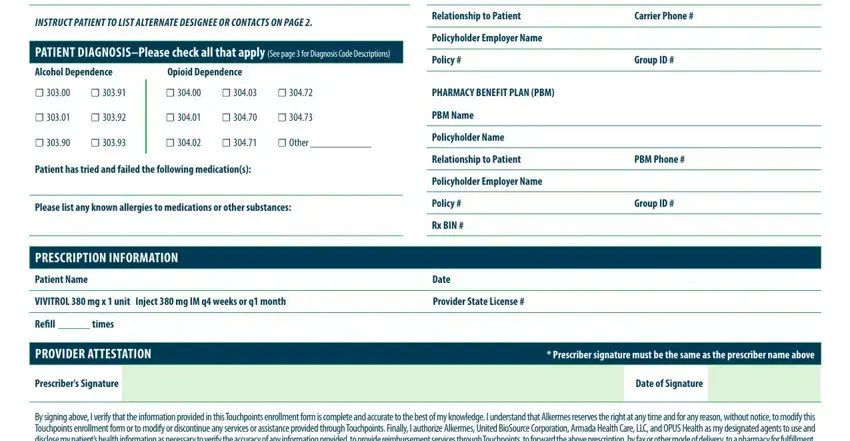
3. The following part focuses on By signing above I verify that the, PLEASE SEE IMPORTANT SAFETY, and PAGE - fill in each one of these blank fields.

Always be extremely mindful when filling in PLEASE SEE IMPORTANT SAFETY and PAGE, as this is where a lot of people make some mistakes.
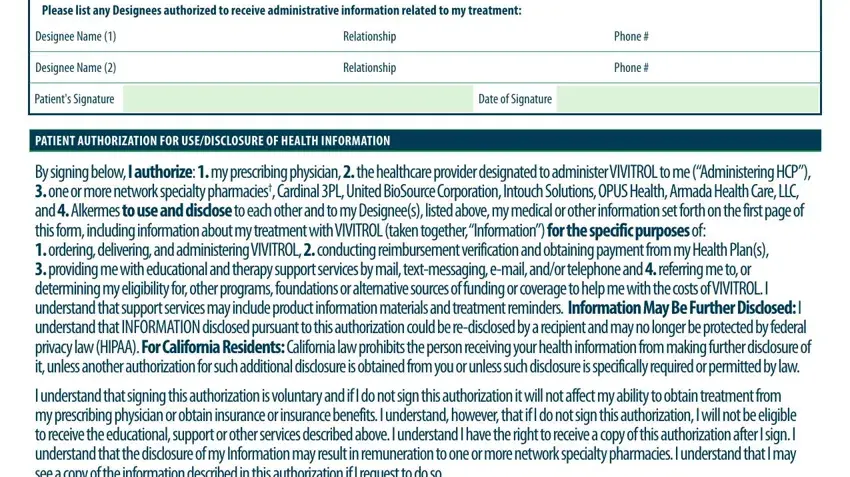
4. You're ready to complete this next part! Here you'll get all of these By signing below I authorize my, Designee Name Relationship Phone, Designee Name Relationship Phone, Patients Signature Date of, PATIENT AUTHORIZATION FOR, By signing below I authorize my, and I understand that signing this blank fields to do.
5. As you get close to the end of the file, you'll notice a few extra things to complete. Mainly, I may withdraw this authorization, Patients Signature Date of, ParentGuardianLegal, Check if yes I would like to, dependence after detox or alcohol, See page for a list of Network, Medicare TRICARE or any other, If patient is a minor without, PLEASE SEE IMPORTANT SAFETY, MEDICATION GUIDE OR VISIT, VIV, and PAGE should be filled in.
Step 3: Immediately after rereading your filled out blanks, press "Done" and you're done and dusted! Try a 7-day free trial option at FormsPal and get immediate access to patient assistance application for vivitrol - download or edit from your personal account. We don't sell or share any information that you use whenever completing forms at our site.