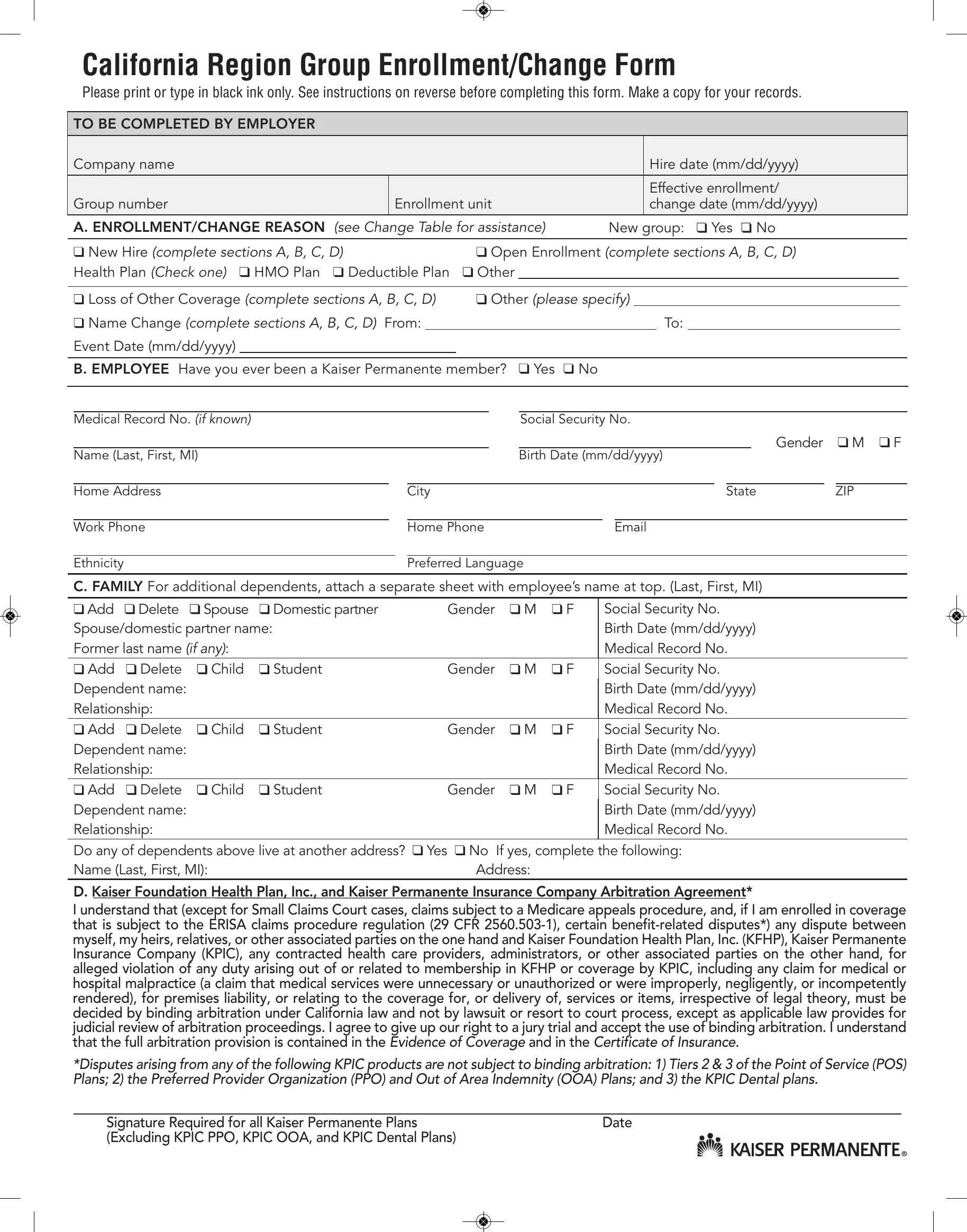
Navigating the Kaiser Enrollment Form is a critical step for employees and employers alike within the California Region, ensuring access to healthcare benefits tailored to their needs. This comprehensive document, designed for the exclusive use of group enrollment or modifications, demands attention to detail, requiring black ink for entries and urging careful review of instructions. It necessitates employer input for foundational information such as company name, hire and effective dates, alongside the employee’s responsibility to specify enrollment or changes, including personal and dependent information. This form covers a broad spectrum of potential changes, from new hires and open enrollment periods to personal events like marriage or the loss of other coverage. Additionally, it addresses specific needs such as the inclusion of dependents, capturing their essential information and any changes in student status or residence that may affect their eligibility. At its core, the Kaiser Enrollment Form binds the signer to Kaiser Permanente's arbitration agreement, waiving the right to resolve disputes through traditional court processes in favor of binding arbitration, a clause with specified exclusions. This document emphasizes not just the procedural aspect of enrolling in healthcare plans but also enshrines the importance of accuracy and clarity in communicating vital information to ensure seamless coverage and understanding of the legal implications embedded in the enrollment process.
| Question | Answer |
|---|---|
| Form Name | Kaiser Enrollment Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | kaiser form online, kaiser permanente account change form california, kaiser form pdf, how to kaiser form |