
DSM can be filled in online very easily. Just make use of FormsPal PDF tool to get the job done in a timely fashion. To make our editor better and simpler to use, we constantly work on new features, with our users' suggestions in mind. In case you are looking to get started, here's what it will take:
Step 1: First of all, access the tool by pressing the "Get Form Button" at the top of this webpage.
Step 2: With the help of our advanced PDF editing tool, you could do more than just fill out blank fields. Express yourself and make your docs appear high-quality with customized textual content added, or adjust the file's original content to excellence - all that accompanied by an ability to insert your personal pictures and sign it off.
This PDF form will require particular data to be filled out, thus you need to take whatever time to type in precisely what is asked:
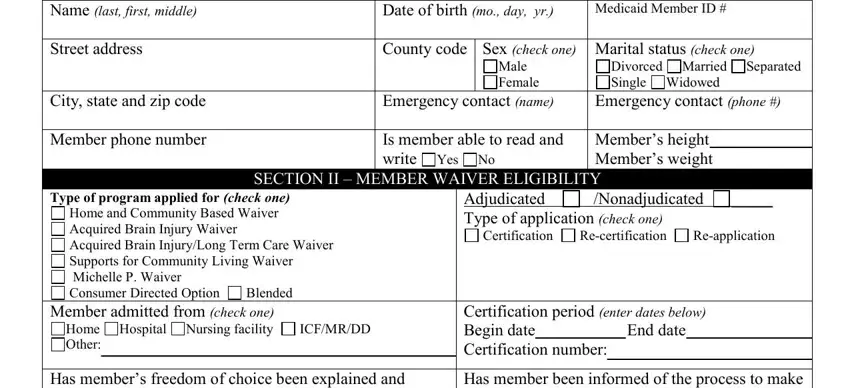
1. When filling in the DSM, make certain to include all of the needed blank fields in its corresponding section. It will help speed up the process, allowing for your details to be handled without delay and properly.
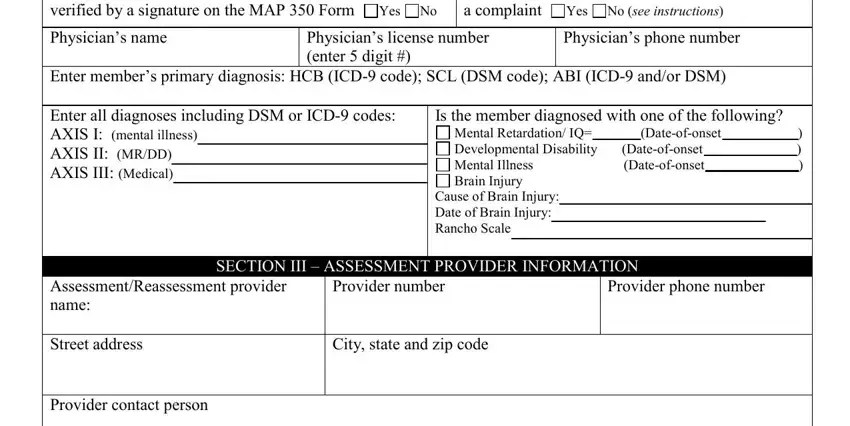
2. Soon after filling in the previous section, go on to the next part and enter the necessary particulars in all these fields - Certification period enter dates, Physicians license number enter, Has members freedom of choice been, Mental Retardation IQ Dateofonset, Is the member diagnosed with one, Physicians phone number, Cause of Brain Injury Date of, SECTION III ASSESSMENT PROVIDER, AssessmentReassessment provider, Provider number, City state and zip code, Provider phone number, and Provider contact person.
3. The following segment is typically rather uncomplicated, Name last first, Medicaid Number, For SCL MP and ABI waivers only, SECTION IV SELF ASSESSMENT, and Community Inclusion what do you - all these fields will have to be completed here.
4. Completing Community Inclusion what do you is paramount in the next section - be sure to spend some time and take a close look at every single empty field!
5. And finally, this last section is precisely what you need to wrap up before closing the document. The blank fields at this point are the following: Name last first, Medicaid Number, SECTION V ACTIVITIES OF DAILY, Comments, Is member independent with, dressingundressing Yes NoIf no, Is member independent with, Yes NoIf no check below all that, Requires handson assistance with, oral care nail care Requires total, shaving hair, Is member independent with bed, Yes No If no check below all that, Is member independent with bathing, and Yes No If no check below all that.
Concerning oral care nail care Requires total and Is member independent with, be certain you do everything correctly here. Both these are the most significant ones in this form.
Step 3: Right after looking through the fields, hit "Done" and you are done and dusted! Download the DSM after you join for a free trial. Easily gain access to the pdf document inside your FormsPal account, along with any modifications and changes all saved! Here at FormsPal, we do our utmost to make sure that all your information is kept private.