Date of Notice:
KEEP FOR YOUR RECORDS
The State of Illinois helps income eligible families pay for their child care services while they work or go to school, training and other work-related activities. To apply please read the following pages carefully and then submit your completed Redetermination to your local Child Care Resource and Referral (CCR&R) or child care center/home if they have a contract with IDHS to provide child care assistance. If you have any questions about your eligibility or if you need help completing this form, call your local CCR&R. To find your local CCR&R go to http://www.inccrra.org/find-your-local-ccrr-other or call 1-877-202-4453 (toll-free).
Please be sure that all of the information is complete before sending in your Redetermination:
*The Redetermination is filled out clearly in blue or black ink.
*All questions on the Redetermination are complete. If the section or question does not apply, write "n/a in the box to show that the question was not missed.
*This information is for your current job/education activity. You will inform the CCR&R or Site provider if any information changes in the future.
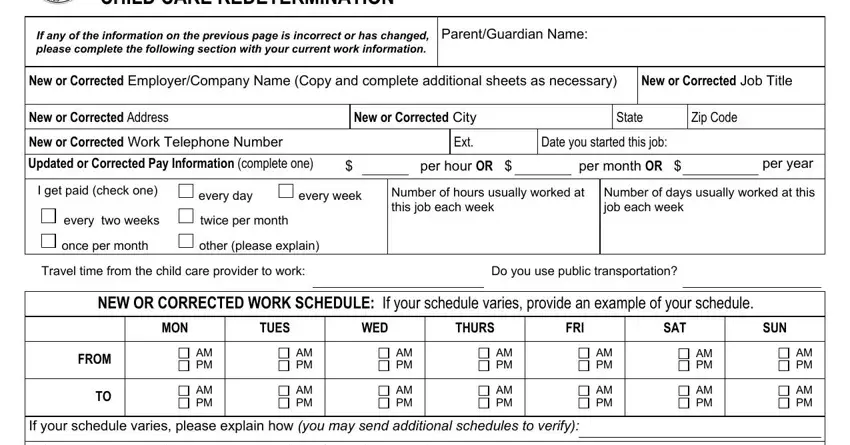
*The parent/guardian's name is listed at the top of each page of the Redetermination.
*Both you and the other parent/adult have signed the Redetermination (page 12).
*All social security numbers are listed clearly or "n/a" is listed in the box. Social security numbers are not required for parents or children but they are used to gather information to help determine your eligibility for child care assistance. All information is confidential and will not be shared with anyone else.
*All Family Information is complete in Section 3 (page 7) including information about your children's immigration status. Children can get assistance regardless of their immigration status, but IDHS is required to ask for this information. This information will not be shared with anyone. Your child's alien registration number must be listed if they have one.
*All persons living in your household are listed in Section 3 (page 7).
*If working, at least one of the following is attached to verify your employment and the employment of everyone listed in your family size that is 19 years of age or older:
**Copies of your last (2) paycheck stubs, or if you have not been working long enough to get two paychecks:
--A letter from your employer or an employment verification form listing the following:
The date you started working.
The amount of money you are paid.
Your typical work schedule, including the total number of hours you work per week.
Your employer's address and phone number.
Your employer's signature, or
**Verification of your self-employment. This can include:
--A copy of your most recent Federal income tax return (IRS 1040) and all schedules and attachments.
--A copy of your quarterly estimated taxes.
--A listing of all business income and expenses for the last 30 days. This can be reported on your own form or on a Self-Employment form which can be downloaded at http://www.dhs.state.il.us/OneNetLibrary/27897 /documents/Forms/IL444-2790.pdf or requested from your local CCR&R. When reporting income and expenses, receipts, invoices, or other documentation must be attached to verify all information.
*If in school, ALL of the following are attached:
**Copies of your official school schedule.
**Copies of your most recent report card showing your cumulative grade point average (GPA).
*You have made a copy of your Redetermination for your records. You understand if you send original check stubs or other documents that they will not be returned.
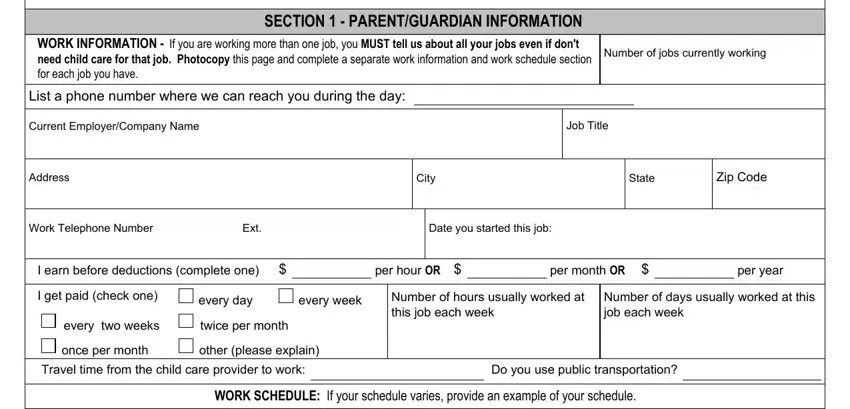
*All jobs and income information for BOTH parents have been reported on pages 3 through 6 and documentation is attached.
*You understand that if any questions are left blank or if any attachments are missing, your redetermination form will be returned to you as incomplete. This may cause a delay in approval for Child Care Assistance Program payments.
*You also understand that all of the information you submit will be verified using State and/or local databases and the internet. If any inconsistencies are discovered, your redetermination may be delayed or your participation in the Child Care Assistance Program may be cancelled.
IL444-3455E (R-6-11) |
Page # of ## |