
Should you would like to fill out quest requisition form, you won't need to install any programs - just use our online tool. Our editor is continually developing to give the very best user experience possible, and that is due to our dedication to constant improvement and listening closely to user comments. All it requires is a few easy steps:
Step 1: Press the "Get Form" button above on this webpage to open our editor.
Step 2: With this state-of-the-art PDF editor, you can actually accomplish more than merely complete blank fields. Edit away and make your documents look professional with custom textual content added, or optimize the file's original content to excellence - all supported by an ability to insert almost any graphics and sign the document off.
In an effort to fill out this PDF document, make sure you enter the required details in every single field:
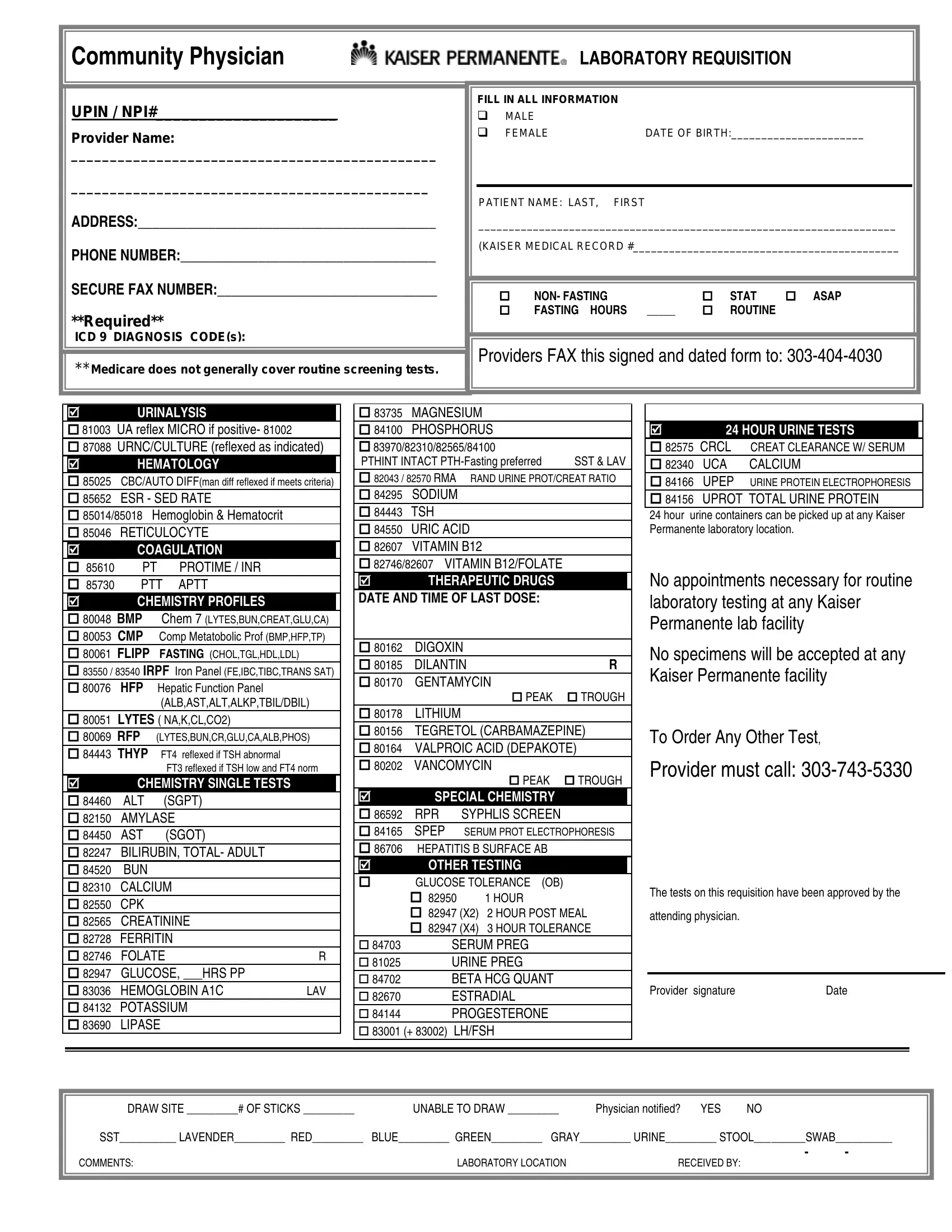
1. When filling in the quest requisition form, make sure to include all of the essential blanks within its relevant form section. This will help speed up the process, allowing your information to be handled without delay and accurately.
2. The next part is to fill out the following fields: COAGULATION LBSP L, PTT APTT CHEMISTRY PROFILES, UA reflex MICRO if positive, R LAV, FT reflexed if TSH low and FT norm, CHEMISTRY SINGLE TESTS, ALBASTALTALKPTBILDBIL, SGOT, SGPT, THERAPEUTIC DRUGS, MAGNESIUM PHOSPHORUS PTHINT, SYPHLIS SCREEN SERUM PROT, SPECIAL CHEMISTRY, PEAK TROUGH, and PEAK TROUGH.
3. This next step is related to UA reflex MICRO if positive, R LAV, HOUR, GLUCOSE TOLERANCE X HOUR POST, SERUM PREG URINE PREG BETA HCG, LHFSH, attending physician, Provider signature, Date, DRAW SITE OF STICKS, For questions regarding tube types, SST LAVENDER RED BLUE GREEN GRAY, UNABLE TO DRAW, LABORATORY LOCATION, and Physician notified - type in every one of these blanks.
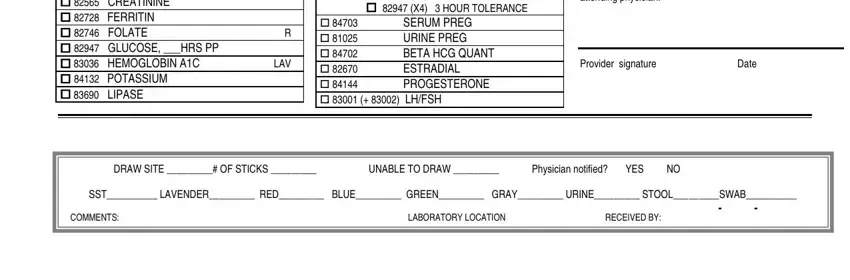
Be extremely attentive when filling in DRAW SITE OF STICKS and HOUR, as this is where many people make mistakes.
Step 3: Always make sure that your details are correct and then just click "Done" to complete the task. Join us now and easily gain access to quest requisition form, set for download. Each change made is conveniently preserved , making it possible to customize the form later on when required. Here at FormsPal.com, we aim to make sure that all your information is maintained protected.