We were designing this PDF editor having the idea of making it as easy to apply as it can be. That's the reason the actual procedure of typing in the lausd hi22 will be simple accomplish the next steps:
Step 1: Select the orange button "Get Form Here" on the webpage.
Step 2: You can now manage your lausd hi22. Our multifunctional toolbar enables you to include, erase, improve, and highlight content material or perhaps undertake other commands.
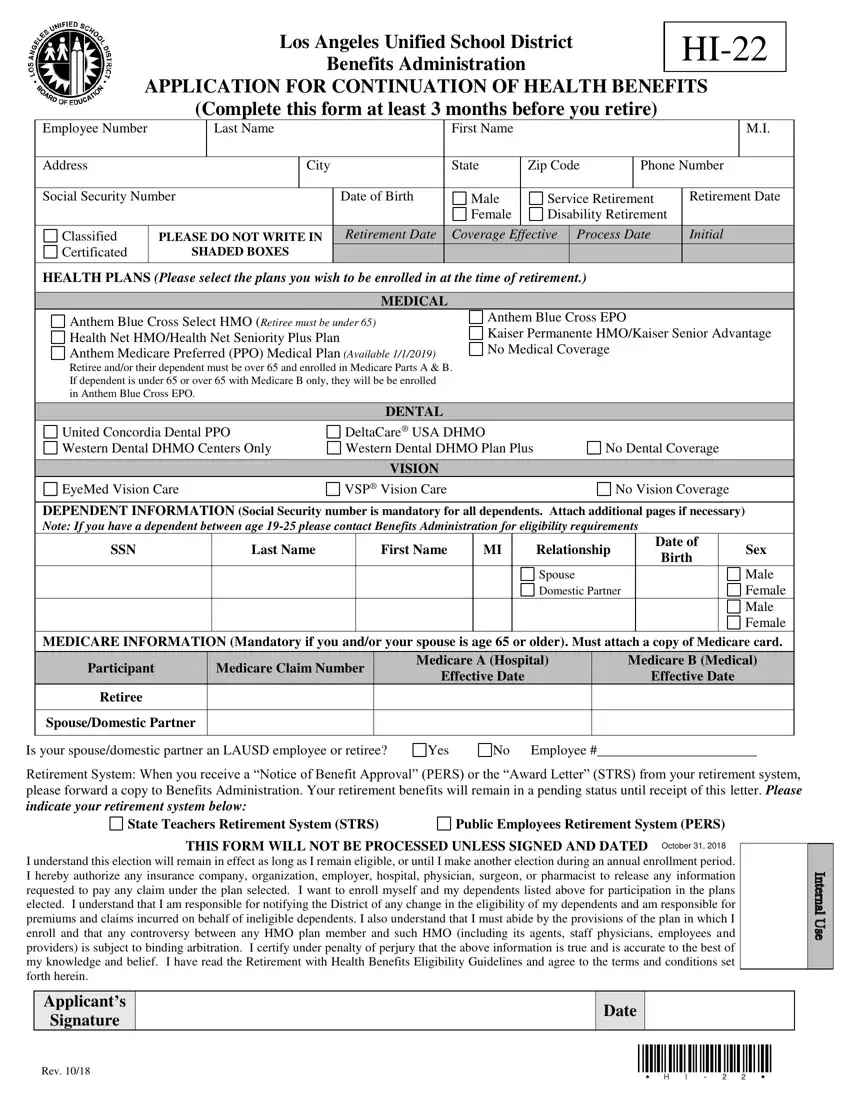
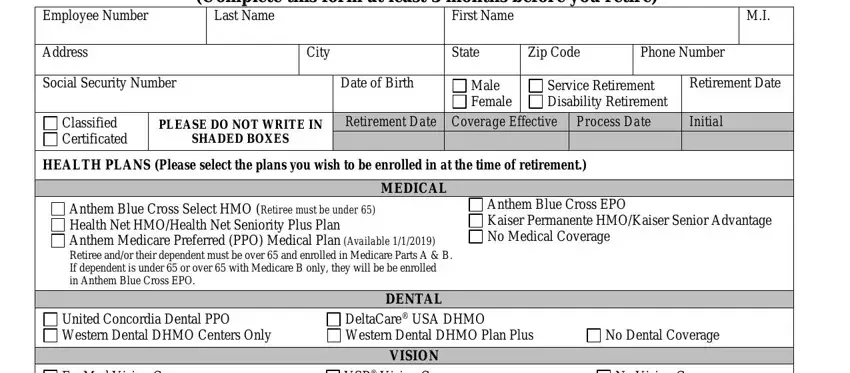
The PDF template you plan to fill in will include the next areas:
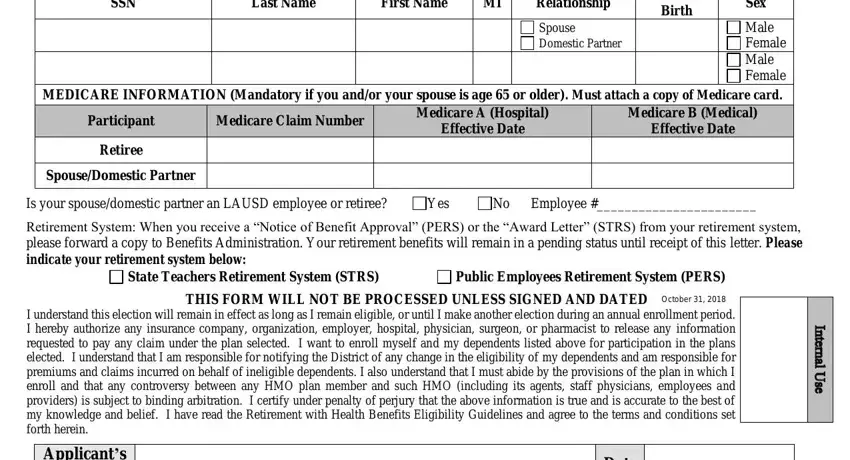
Within the section SSN, Last Name, First Name, Relationship, Date of Birth, Sex, Male Female Male Female MEDICARE, Spouse Domestic Partner, Participant, Medicare Claim Number, Medicare A Hospital Effective Date, Medicare B Medical Effective Date, Retiree, SpouseDomestic Partner, and Is your spousedomestic partner an enter the data that the platform demands you to do.
Put down the valuable particulars when you find yourself on the Los Angeles Unified School area.

Step 3: Choose the Done button to confirm that your finished form may be exported to every gadget you end up picking or delivered to an email you specify.
Step 4: Come up with as much as two or three copies of your file to remain away from any specific potential future troubles.
