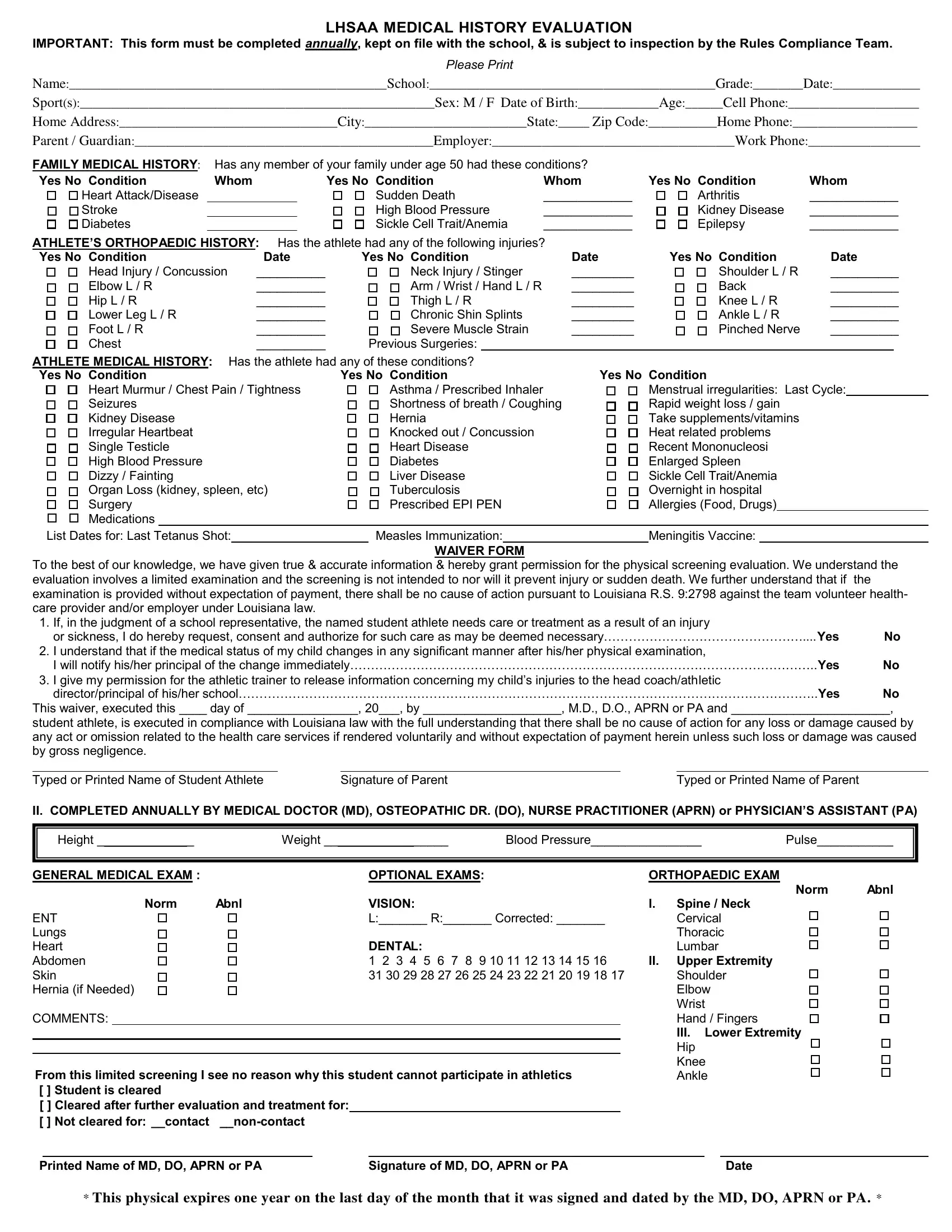
The LHSAA Medical History Evaluation form is a crucial document designed to safeguard the health and safety of student athletes by gathering comprehensive health information annually. This requirement not only facilitates a better understanding of the student's medical and orthopedic history but also establishes a baseline for monitoring potential health risks associated with sports participation. The form covers a wide range of details, from personal and family medical history to specifics about prior injuries and conditions that may impact the student's ability to engage safely in sports activities. Additionally, it outlines the conditions under which emergency medical treatment can be authorized, ensuring that swift and appropriate measures can be taken in the event of an injury or sickness. The waiver section further details the legal understanding between the student athlete, their guardian, and the volunteer healthcare provider, highlighting the limited nature of the physical screening and the specific legal protections in place for volunteers under Louisiana law. By requiring a detailed account of the athlete's medical background and current health status, completed and updated annually, this form plays a vital role in preventive health measures and in promoting a safe sporting environment.
| Question | Answer |
|---|---|
| Form Name | Lhsaa Medical History Evaluation Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | lhsaa medical history evaluation, lhsaa medical history evaluation 2021, lhsaa medical, lhsaa medical history evaluation form |