It shouldn’t be challenging to create la oaas locet through our PDF editor. This is the way one could conveniently prepare your document.
Step 1: You should hit the orange "Get Form Now" button at the top of this page.
Step 2: You are now allowed to update la oaas locet. You've got lots of options thanks to our multifunctional toolbar - it's possible to add, eliminate, or modify the content, highlight the specified areas, as well as perform similar commands.
Fill in all of the following areas to fill out the template:
Jot down the details in Home Tel, Facility Name if known, Parish, Mailing Address if different from, Name, Address, Address, City State Zip, D Other Contact Information, Type of Other Contact Personal, Name, Address, Address, City State Zip, and Telephone.
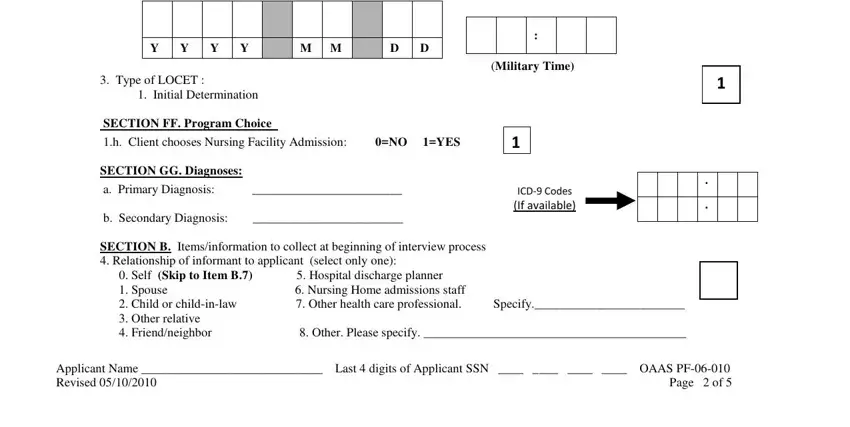
The system will ask you for details to quickly fill in the segment Applicant Name Last digits of.

The b The information I provide will, No Yes, c The results of this interview, No Yes, d The Louisiana Department of, No Yes, e All program requirements must be, No Yes, Informant indicates that, Date, ACSRO Users SKIP TO SECTION EE, SECTION EE Initial Call and LOCET, and DateTime LOCET Initiated area will be your place to insert the rights and obligations of all parties.
Finish by looking at the following sections and filling them out as required: DateTime LOCET Initiated, Y Y Y Y, M M, D D, Military Time Type of LOCET, SECTION FF Program Choice h, SECTION GG Diagnoses a Primary, b Secondary Diagnosis, ICD Codes If available, SECTION B Itemsinformation to, and Applicant Name Last digits of.
Step 3: Choose the Done button to be certain that your completed document could be exported to every gadget you decide on or mailed to an email you indicate.
Step 4: Generate copies of your file - it may help you keep away from possible future complications. And don't be concerned - we don't display or watch your data.
