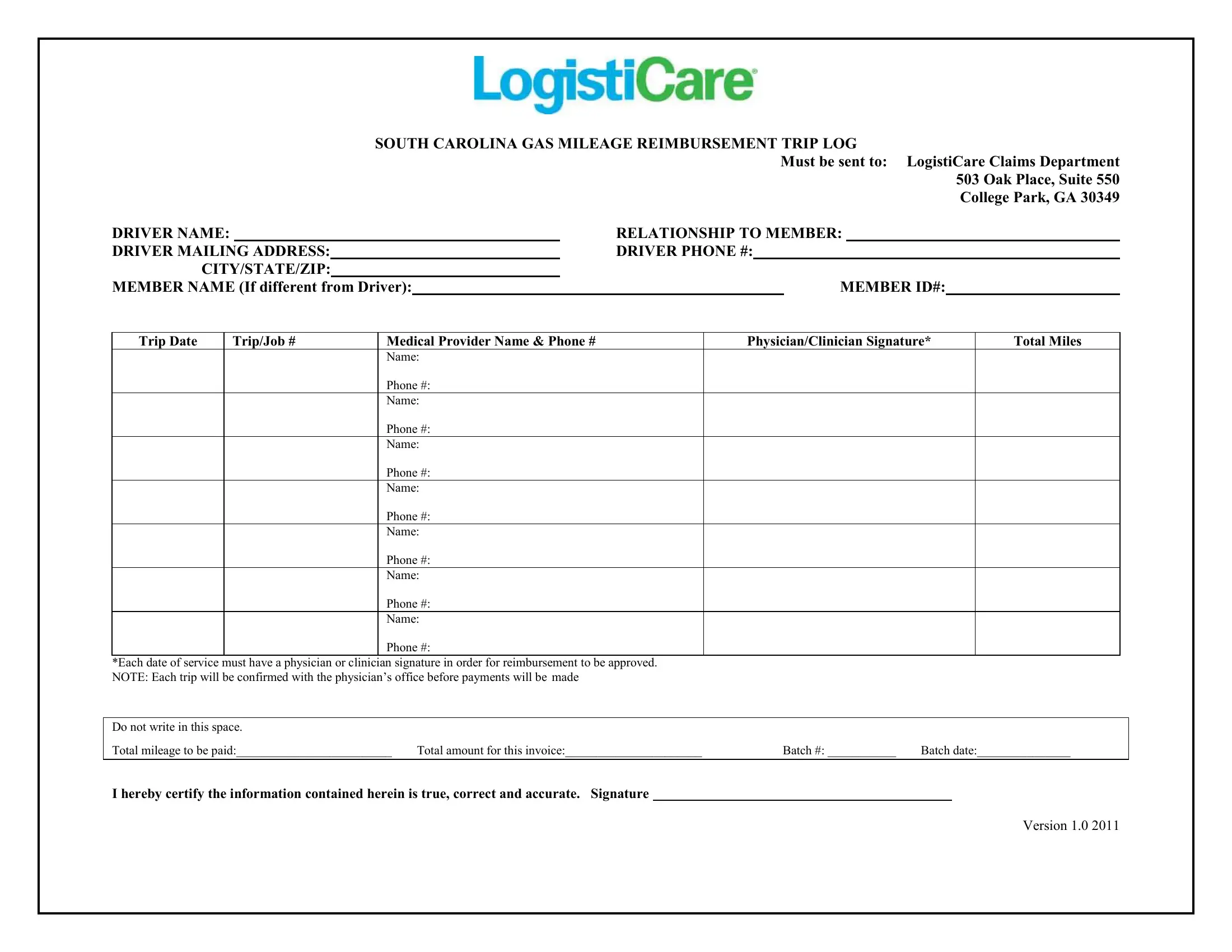
When residents of South Carolina find themselves needing to travel for medical appointments, the Logisticare Gas Mileage Reimbursement Trip Log emerges as a crucial form, streamlining the process of seeking fuel cost recompenses. This document, diligently designed to be sent to the LogistiCare Claims Department in College Park, Georgia, ensures that individuals who drive themselves or others for medical services can recuperate some of the transportation expenses incurred. With spaces provided for extensive details such as the driver's name, their relationship to the member, contact information, and the specifics of each trip, including dates, job numbers, medical provider details, and the mileage covered, it encapsulates all necessary data to facilitate a smooth reimbursement process. Crucially, the form mandates the endorsement of a physician or clinician for each service date, underscoring the authenticity of the travel claim. A noteworthy point is the verification step by LogistiCare, wherein each trip is confirmed with the respective physician's office before any payment is processed, adding an extra layer of validation. Embodying a straightforward yet pivotal document, the Logisticare Gas Mileage Reimbursement Trip Log reflects an understanding of the financial burdens that can accompany medical care, offering a method to alleviate some of these stresses for South Carolinians.
| Question | Answer |
|---|---|
| Form Name | Logisticare Gas Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | logisticare, sc gas mileage, south carolina reimbursement, logisticare gas reimbursement |