Filling in mq11 form is straightforward. We developed our tool to make it intuitive and assist you to complete any PDF online. Here are a few steps that you need to go through:
Step 1: You can choose the orange "Get Form Now" button at the top of this page.
Step 2: It's now possible to modify the mq11 form. The multifunctional toolbar lets you insert, eliminate, modify, and highlight content or undertake other commands.
The next areas will compose the PDF template that you will be creating:
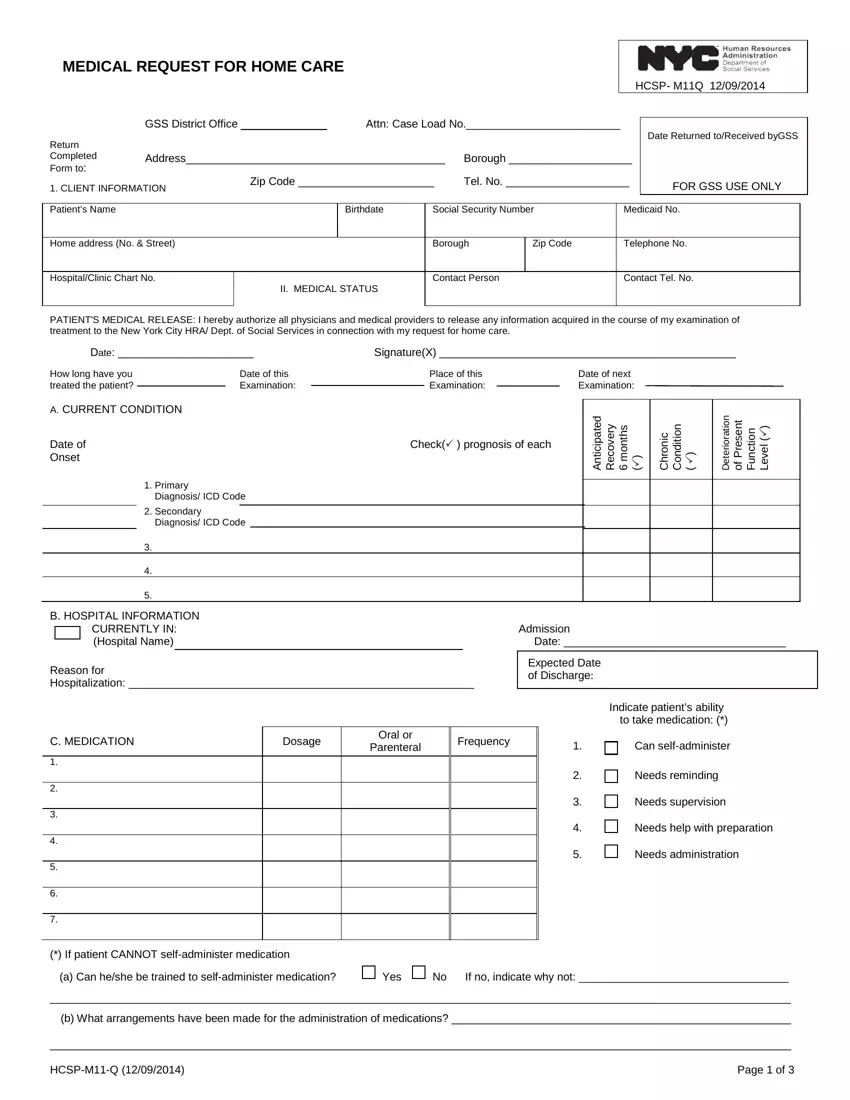
In the Primary Diagnosis ICD Code, B HOSPITAL INFORMATION CURRENTLY, Admission Date, Reason for Hospitalization, Expected Date of Discharge, Indicate patients ability to take, C MEDICATION, Dosage, Oral or Parenteral, Frequency, Can selfadminister, Needs reminding, Needs supervision, Needs help with preparation, and Needs administration field, type in your data.
The application will demand you to give particular vital particulars to effortlessly submit the field b What arrangements have been made, and HCSPMQ Page of.

The D MEDICAL TREATMENT, Does the patient receive any of, Yes No, Decubitus Care, Dressings Sterile, Simple, Bed bound Care turning, exercising positioning, Ambulation Exercise, ROMTherapeutic Exercise, Enema, Colostomy Care, Ostomy Care, Oxygen Administration, and Catheter Care section can be used to specify the rights and obligations of either side.
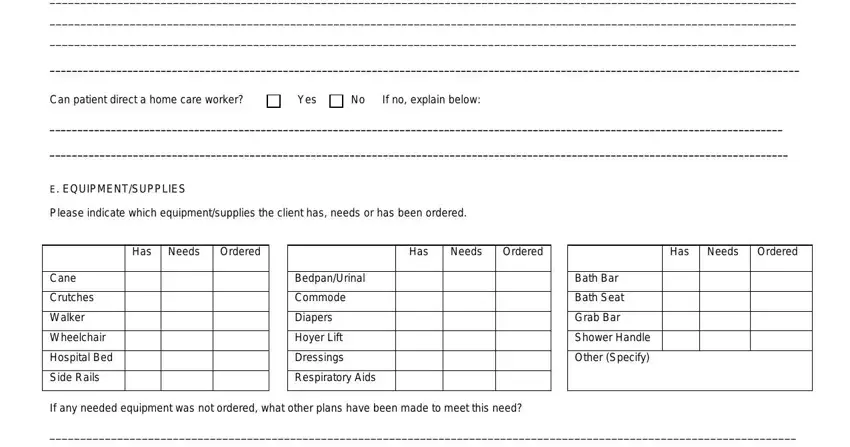
Complete the form by looking at all of these areas: Please indicate contributing, Can patient direct a home care, Yes No, If no explain below, E EQUIPMENTSUPPLIES, Please indicate which, Has Needs Ordered, Has, Needs Ordered, Has Needs Ordered, Cane, Crutches, Walker, Wheelchair, and Hospital Bed.
Step 3: As soon as you are done, click the "Done" button to transfer the PDF file.
Step 4: Get duplicates of the template. This may save you from upcoming complications. We cannot check or share the information you have, thus be certain it will be safe.
