

 15 Moped
15 Moped
 16 Low Speed
16 Low SpeedThis form is required for documenting motor vehicle accidents in Massachusetts under certain circumstances, such as when there is injury, death, or significant property damage.
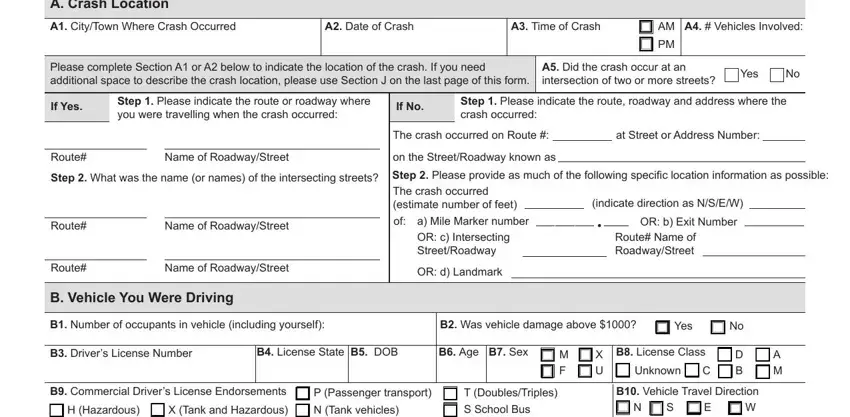
1. Document Crash Location
In Section A, specify the crash location with details like city, street names, and landmarks, ensuring the description is precise enough for exact identification.
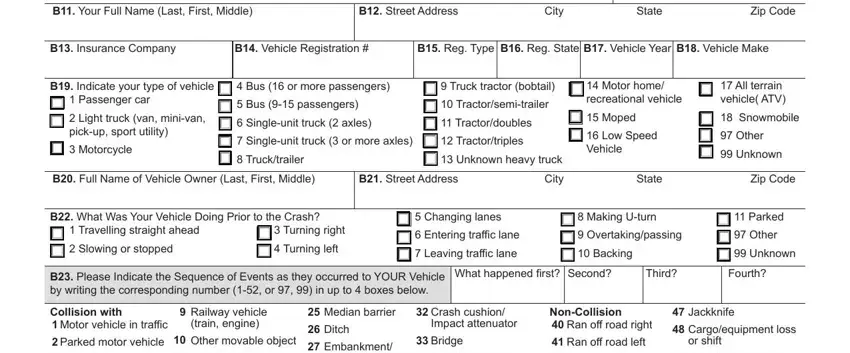
2. Describe Your Vehicle and Incident
In Section B, provide full details of your vehicle and describe your actions and the vehicle's direction prior to the crash.
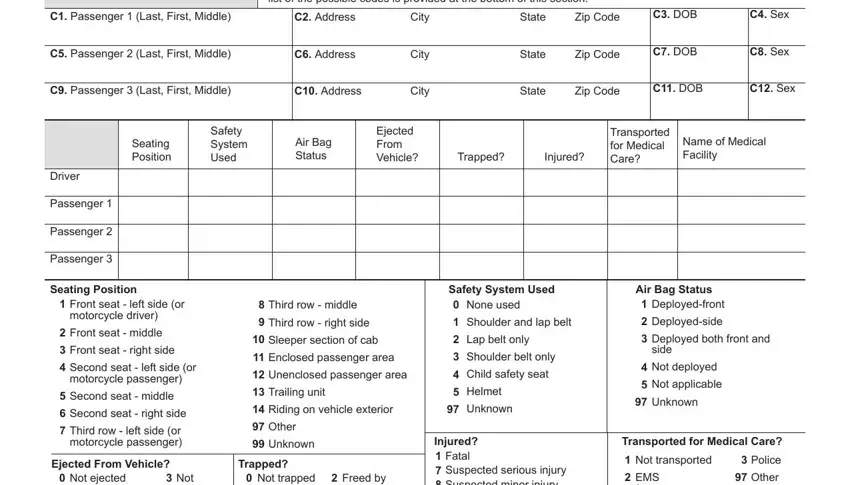
3. Information on All Parties
Record personal and injury details for yourself and any passengers in Section C. Repeat for other vehicles and non-motorists involved in Sections D and E.
4. Note Crash Conditions
In Section F, detail environmental conditions at the crash time, including weather, lighting, and road surface.
5. Provide a Crash Diagram
Create a diagram in Section G showing vehicle positions, directions of travel, and impacts, which aids in claims and legal evaluations.
The Work zone maintenance equipment, Guardrail, B Was your Vehicle Towed from the, Yes, B Vehicle Damaged Area check up to, None, Undercarriage, Totaled, Other, Unknown, and CRASH field needs to be used to list the rights or responsibilities of both parties.

6. Witness Details
List all witnesses with their contact information in Section H, as their accounts can be crucial for further proceedings.
7. Report Property Damage
If applicable, detail any property damage other than to vehicles in Section I, including descriptions and estimated repair costs.
8. Narrative Description of the Crash
Offer a detailed account of the crash in Section J, including events leading up to and during the incident, covering all involved parties and vehicles.
9. Sign and Date
Finalize the form in Section K with your signature and date, verifying the accuracy and truthfulness of the information provided.
