
When using the online PDF tool by FormsPal, you are able to fill in or edit form md 100 right here and now. The tool is consistently improved by our team, receiving cool functions and becoming greater. With just a few simple steps, you are able to start your PDF journey:
Step 1: Hit the "Get Form" button in the top part of this webpage to get into our editor.
Step 2: After you access the online editor, you will notice the form prepared to be filled in. Besides filling in different blank fields, you may also do other things with the PDF, that is adding custom words, changing the original textual content, adding illustrations or photos, putting your signature on the form, and more.
In an effort to complete this PDF form, make sure that you type in the information you need in every single area:
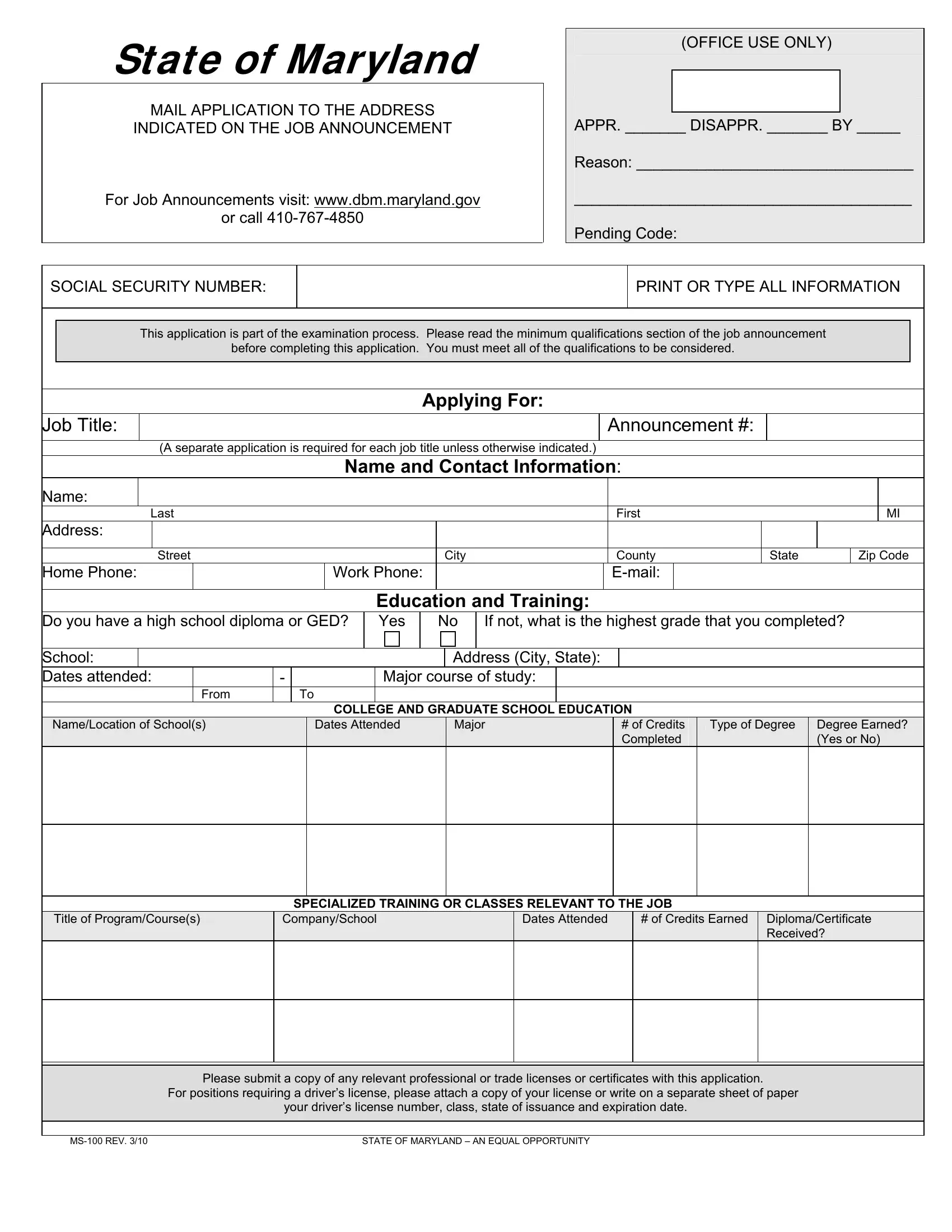
1. It is very important complete the form md 100 properly, hence take care when working with the segments that contain these blank fields:
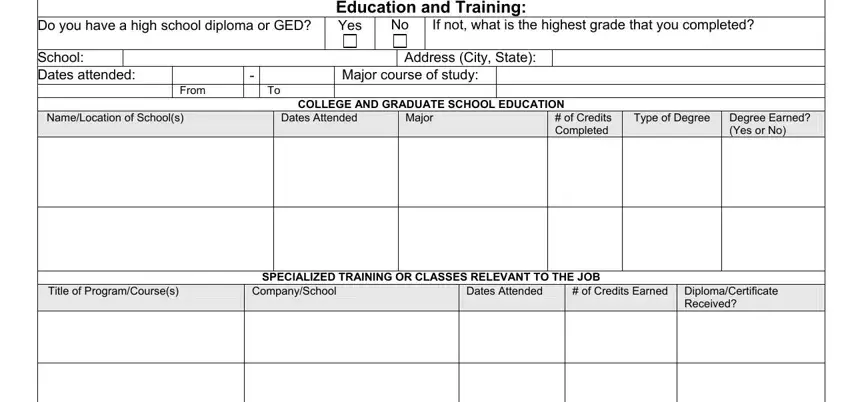
2. The subsequent stage is usually to fill in all of the following fields: Do you have a high school diploma, School Dates attended, From, If not what is the highest grade, Education and Training Yes, No Address City State, Major course of study, COLLEGE AND GRADUATE SCHOOL, NameLocation of Schools, Dates Attended, Major, of Credits Completed, Type of Degree, Degree Earned Yes or No, and Title of ProgramCourses.
3. Completing Name of Employer, Type of Business, Your Job Title, Employers Address Street City, Supervisors Name and Phone Number, Do you supervise other employees, How many, Job Titles of Those You Supervise, Dates of Employment From, Is your position considered, Job Duties, How many hours do you work per week, Reason For Leaving, Job Number, and Name of Employer is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
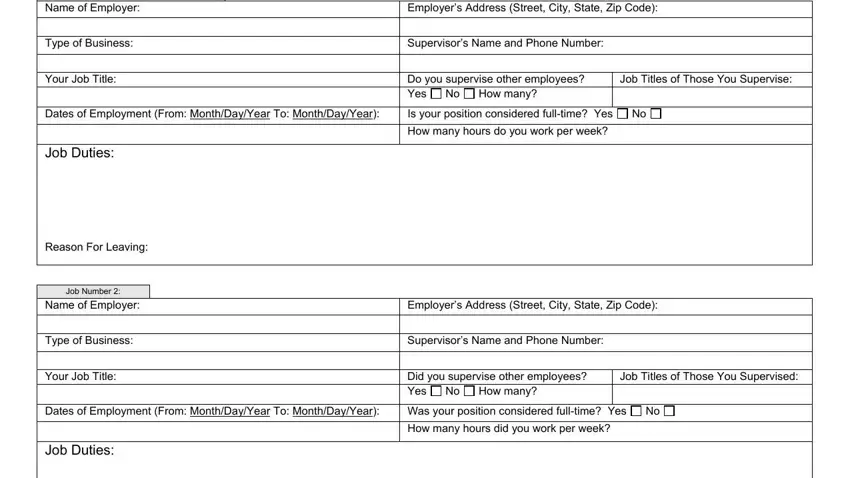
It is possible to make a mistake when filling out the Your Job Title, consequently be sure you take another look prior to deciding to send it in.
4. To move onward, the next step involves filling out several form blanks. Examples include Reason For Leaving, Job Number, Name of Employer, Type of Business, Your Job Title, Employers Address Street City, Supervisors Name and Phone Number, Did you supervise other employees, How many, Job Titles of Those You Supervised, Dates of Employment From, Was your position considered, Job Duties, Reason For Leaving, and How many hours did you work per, which are key to going forward with this particular process.
5. And finally, this final part is precisely what you should complete before using the PDF. The blanks at this point are the following: Employers Address Street City, Supervisors Name and Phone Number, Did you supervise other employees, How many, Job Titles of Those You Supervised, Name of Employer, Type of Business, Your Job Title, Dates of Employment From, Was your position considered, Job Duties, Reason For Leaving, Job Number, Name of Employer, and Type of Business.
Step 3: Prior to finalizing the document, make sure that all blank fields are filled in right. When you’re satisfied with it, click “Done." Try a 7-day free trial plan at FormsPal and obtain immediate access to form md 100 - with all changes preserved and available inside your personal account page. FormsPal ensures your information confidentiality with a secure method that in no way records or distributes any type of private information involved in the process. Be assured knowing your paperwork are kept protected any time you use our editor!