
It is really straightforward to fill out the molst form massachusetts empty blanks. Our PDF tool will make it pretty much effortless to edit any type of PDF. Down the page are the primary four steps you should consider:
Step 1: Choose the button "Get Form Here" on the following website and press it.
Step 2: After you have accessed the editing page molst form massachusetts, you should be able to notice every one of the options intended for your document in the top menu.
The following sections are going to make up your PDF file:
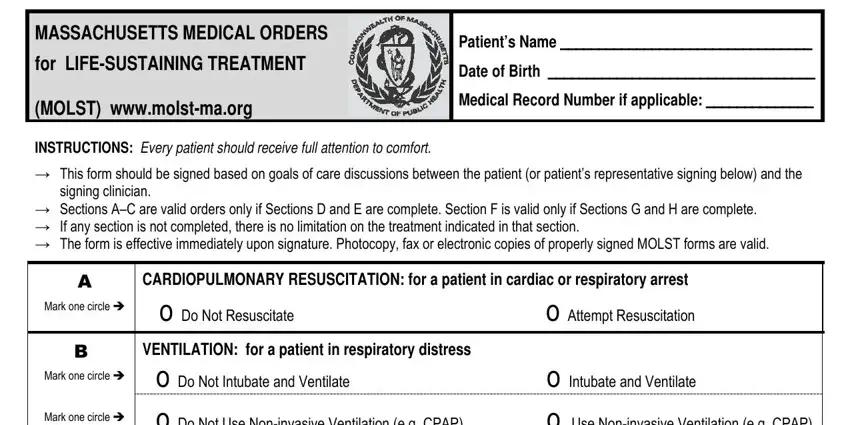
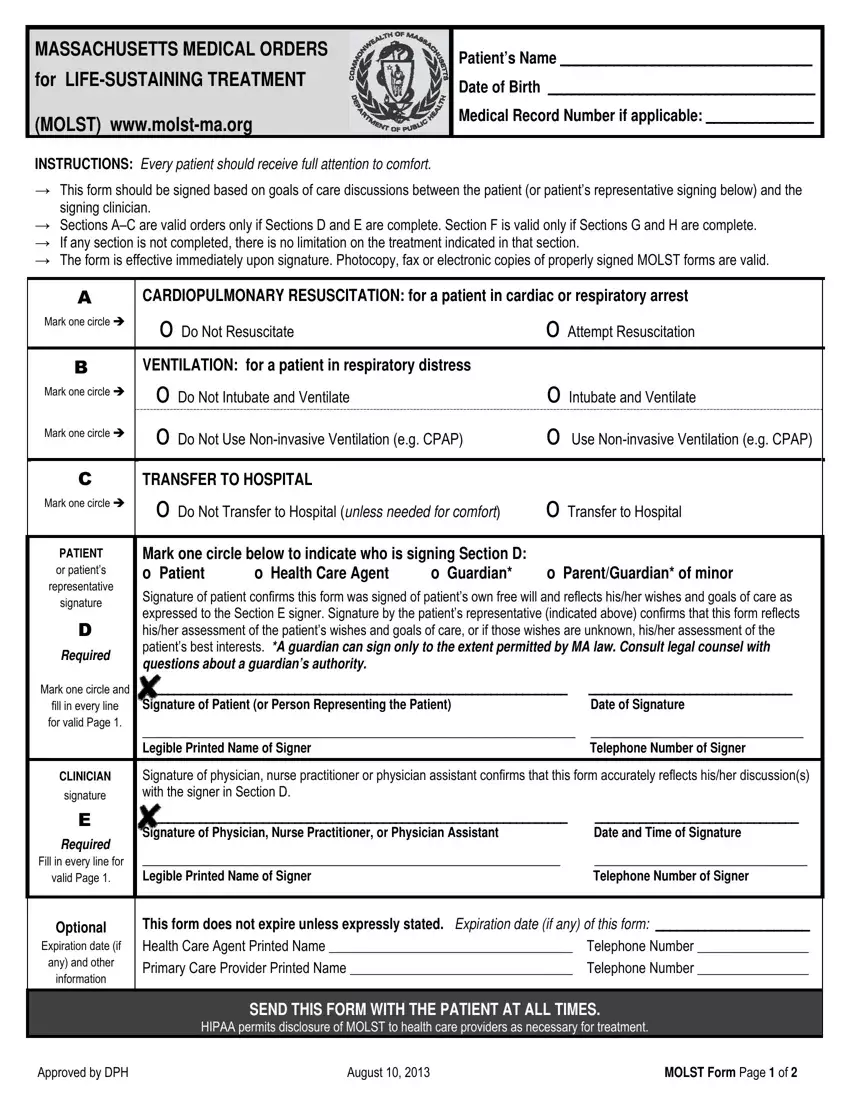
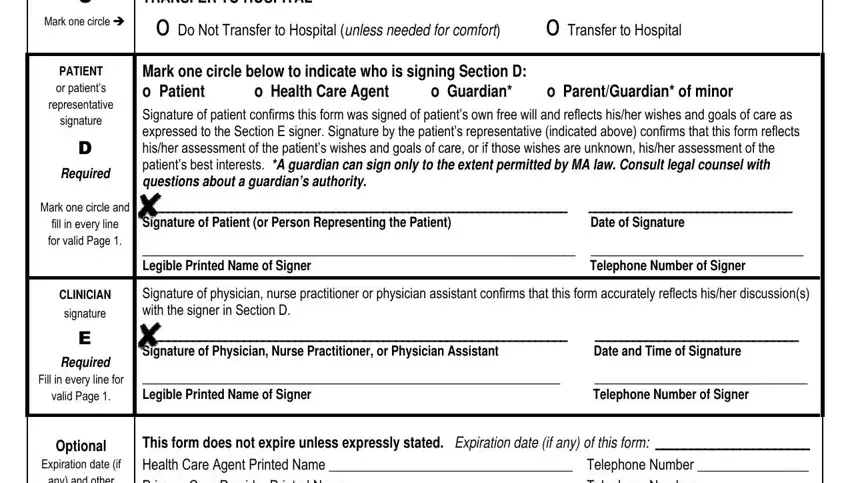
Please provide the appropriate data in the C Mark one circle cid, TRANSFER TO HOSPITAL o Do Not, PATIENT or patients representative, Required, Mark one circle below to indicate, Mark one circle and fill in every, CLINICIAN signature, E Required Fill in every line for, Optional Expiration date if any, Signature of Patient or Person, Legible Printed Name of Signer, Signature of physician nurse, Signature of Physician Nurse, Legible Printed Name of Signer, and This form does not expire unless field.
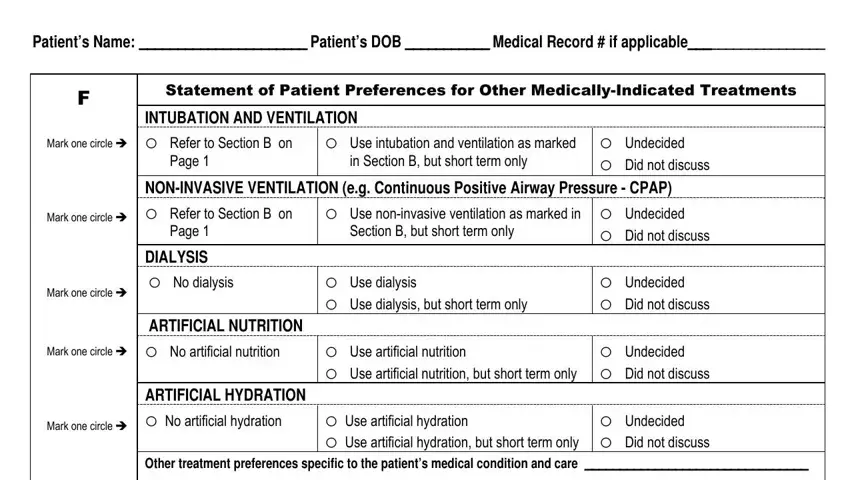
Write down the obligatory data once you are within the Patients Name Patients DOB, Mark one circle cid, Mark one circle cid, Statement of Patient Preferences, INTUBATION AND VENTILATION o Refer, Page, o Use intubation and ventilation, o Undecided o Did not discuss, NONINVASIVE VENTILATION eg, o Use noninvasive ventilation as, Section B but short term only, Page, DIALYSIS o No dialysis, Mark one circle cid, and Mark one circle cid field.
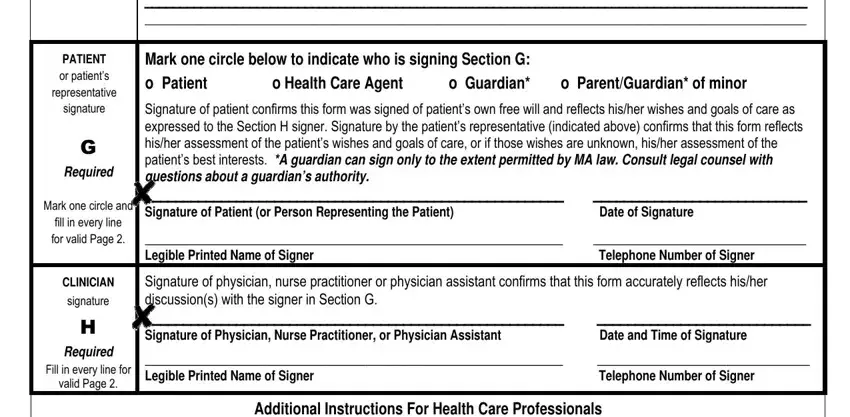
The Other treatment preferences, PATIENT or patients representative, G Required, Mark one circle and fill in every, CLINICIAN signature, H Required Fill in every line for, Mark one circle below to indicate, Signature of patient confirms this, Legible Printed Name of Signer, Signature of physician nurse, and Additional Instructions For Health box enables you to indicate the rights and responsibilities of both parties.
Finish by analyzing the following fields and writing the relevant details: Access the Clinician Checklist, Listen to MOLST Overview for, Access the MOLST website at, For more information about, httpwwwmolstmaorg, Astrobrights Pulsar Pink paper, Staples Item Wausau Astrobrights, Office Depot Item Astrobrights, August, and MOLST Instructions Page of.
Step 3: Once you choose the Done button, your ready form can be easily exported to all of your devices or to electronic mail specified by you.
Step 4: In avoiding potential forthcoming challenges, ensure that you possess minimally two or three duplicates of each form.
