
It is possible to fill out Numident easily in our PDFinity® online tool. FormsPal team is committed to providing you with the perfect experience with our editor by consistently presenting new capabilities and improvements. Our tool has become even more useful thanks to the latest updates! Now, filling out PDF files is simpler and faster than ever before. With some simple steps, it is possible to start your PDF editing:
Step 1: Click on the "Get Form" button in the top section of this webpage to get into our tool.
Step 2: With our handy PDF tool, you can do more than simply fill out blank fields. Express yourself and make your docs appear professional with customized text added in, or adjust the file's original input to perfection - all comes with the capability to add any type of pictures and sign the file off.
This form requires specific information to be filled out, so ensure you take your time to enter what's required:
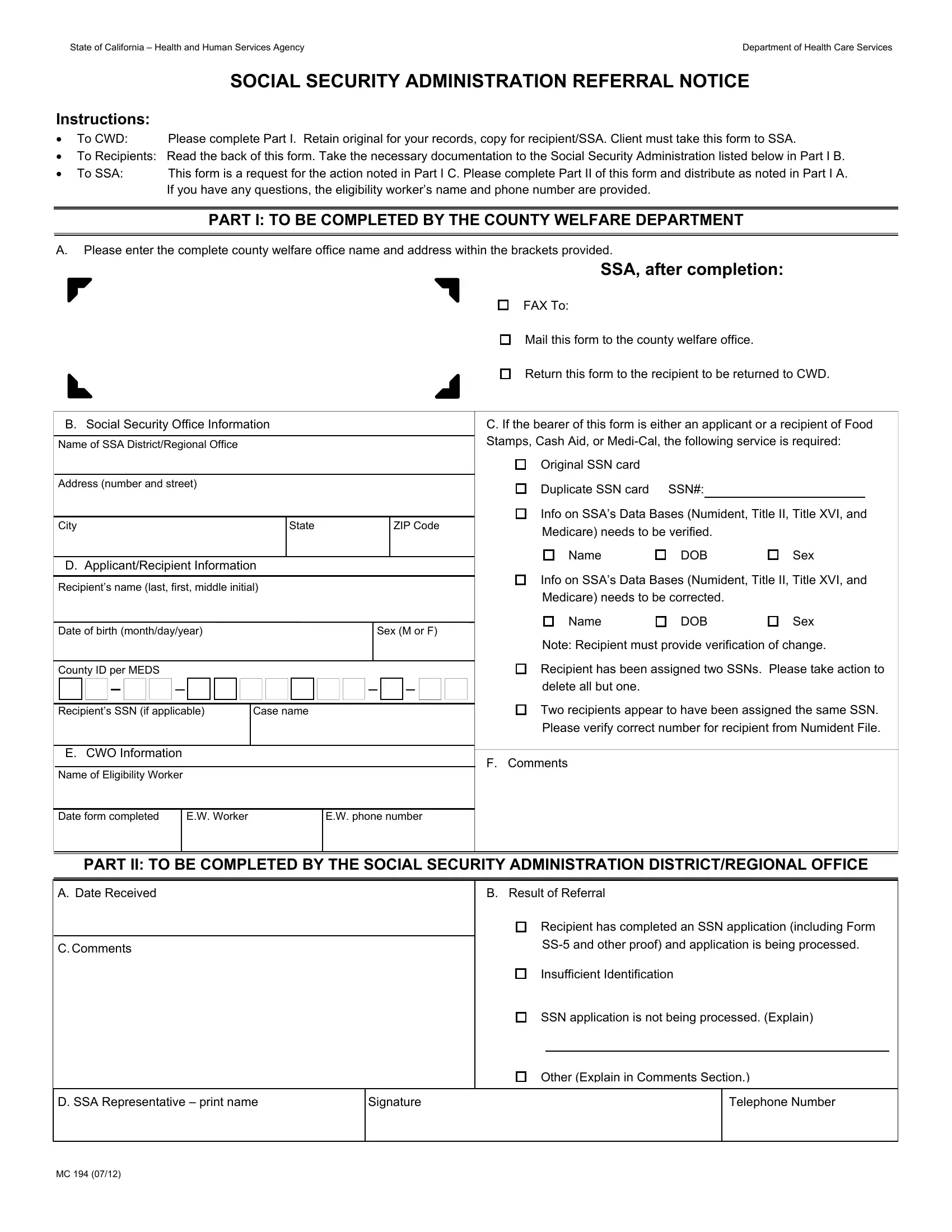
1. Fill out your Numident with a group of necessary blank fields. Gather all the important information and make certain nothing is overlooked!
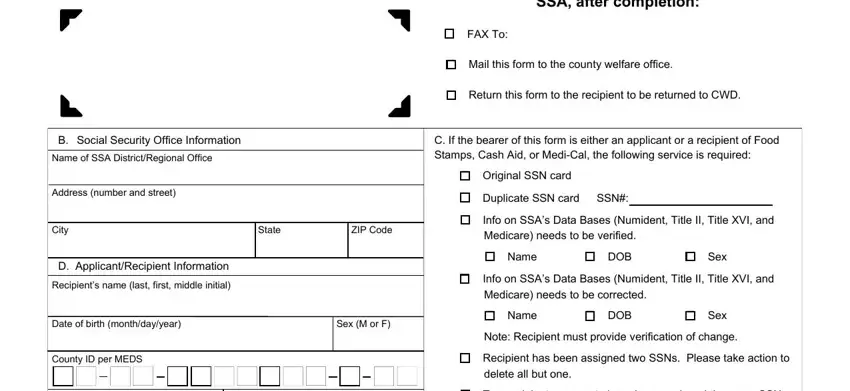
2. Once this part is done, go to enter the suitable details in these - B Social Security Office, Recipients SSN if applicable Case, E CWO Information Name of, EW phone number, Info on SSAs Data Bases Numident, F Comments, PART II TO BE COMPLETED BY THE, A Date Received, CComments, B Result of Referral, Recipient has completed an SSN, Insufficient Identification, SSN application is not being, Other Explain in Comments Section, and D SSA Representative print name.
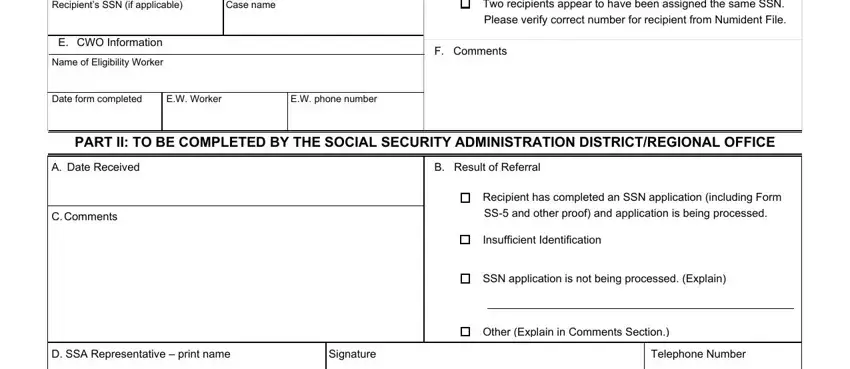
People often make errors when filling in PART II TO BE COMPLETED BY THE in this section. Remember to double-check what you type in right here.
Step 3: Check what you've entered into the blank fields and click on the "Done" button. Go for a free trial option with us and gain instant access to Numident - download, email, or change from your personal account page. FormsPal offers risk-free document completion without personal information record-keeping or any type of sharing. Rest assured that your information is safe here!