We chose the top-rated software engineers to make the PDF editor. Our software will let you fill out the additional family members form with no trouble and won't eat up too much of your time and effort. This simple guide may help you begin.
Step 1: Hit the orange button "Get Form Here" on the web page.
Step 2: So, it is possible to alter your additional family members. This multifunctional toolbar will let you add, eliminate, alter, highlight, and also conduct similar commands to the words and phrases and areas within the file.
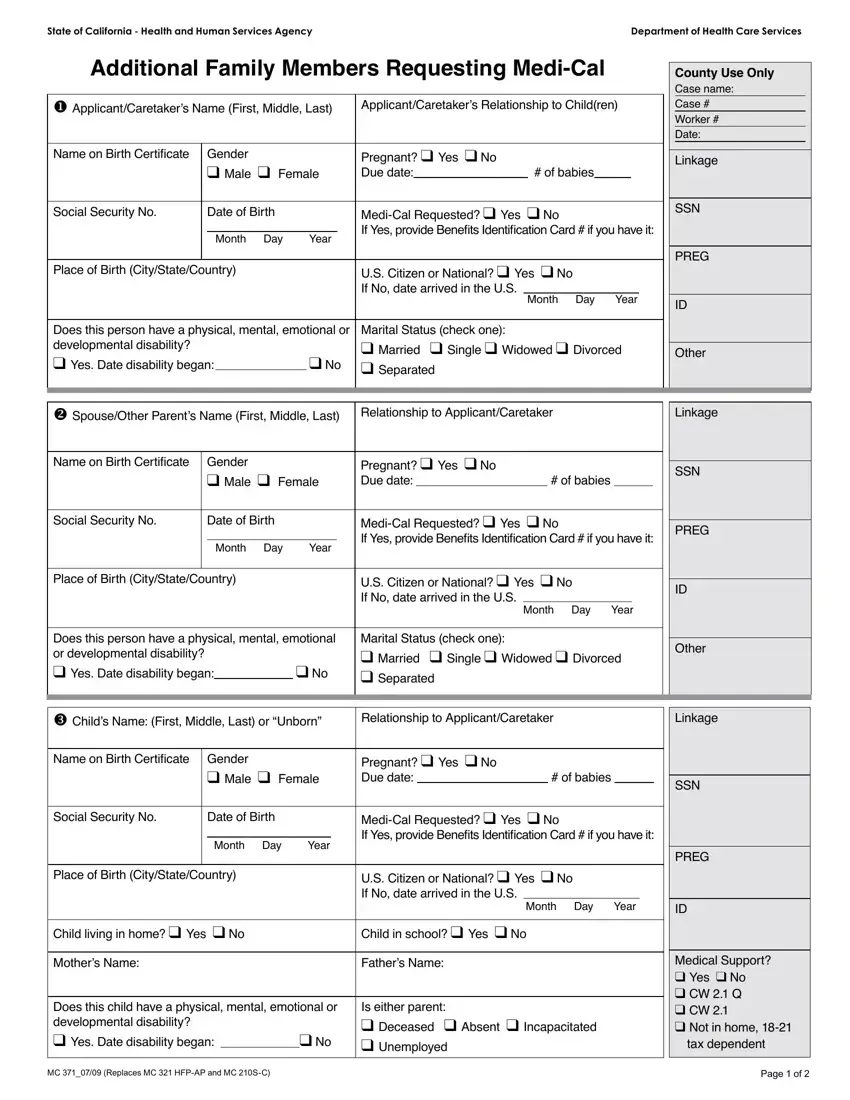
Prepare the additional family members PDF by typing in the information required for every section.
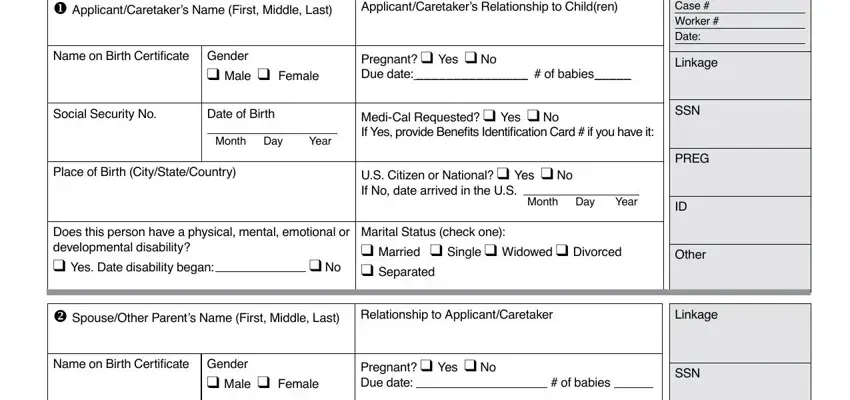
Fill in the Social Security No, Date of Birth, Month Day Year, MediCal Requested q Yes q No If, PREG, Place of Birth CityStateCountry, US Citizen or National q Yes q No, Month Day Year, Does this person have a physical, Marital Status check one q Married, Other, w Childs Name First Middle Last or, Relationship to ApplicantCaretaker, Linkage, and Name on Birth Certiicate Gender field with all the data asked by the software.
Make sure you highlight the essential data in the Mothers Name, Fathers Name, Does this child have a physical, Is either parent q Deceased q, MC Replaces MC HFPAP and MC SC, Medical Support q Yes q No q CW Q, and Page of part.

You'll need to define the rights and responsibilities of both parties in section x Is anyone currently covered by, q DHCS, If so who, OHC Code, y Has anyone iled a lawsuit, q DHCS, z Do you or any family member want, q MC A, and wish to apply for MediCal q, List names Months of coverage, Retroactive Coverage, Month Month Month, Have you or any family member, q CW, and If Yes who Names.
End by looking at the following sections and filling in the pertinent information: Name of person with Income, Source of Income Job social, How often is income received, How much is the income Total gross, Social Security No Optional, Expenses List the monthly, Child Day Care or Disabled, For child or dependents name Age, How Often, For child or dependents name Age, How Often, Courtordered child support Paid to, Courtordered spousal support Paid, Please note that additional, and I certify that I have read and.
Step 3: Select the Done button to be certain that your finalized form is available to be transferred to every gadget you end up picking or delivered to an email you specify.
Step 4: You can generate duplicates of the document tokeep clear of any kind of upcoming challenges. Don't get worried, we don't display or watch your details.
