







Using PDF documents online is certainly super easy with this PDF tool. Anyone can fill out medicaid threshold override form here and try out a number of other functions available. FormsPal professional team is ceaselessly working to enhance the tool and help it become even easier for users with its extensive functions. Uncover an endlessly progressive experience today - explore and uncover new possibilities along the way! To begin your journey, go through these easy steps:
Step 1: Press the "Get Form" button in the top area of this webpage to get into our PDF editor.
Step 2: This editor offers you the capability to change the majority of PDF forms in a variety of ways. Change it by including customized text, correct original content, and place in a signature - all at your disposal!
As for the blank fields of this precise document, this is what you need to do:
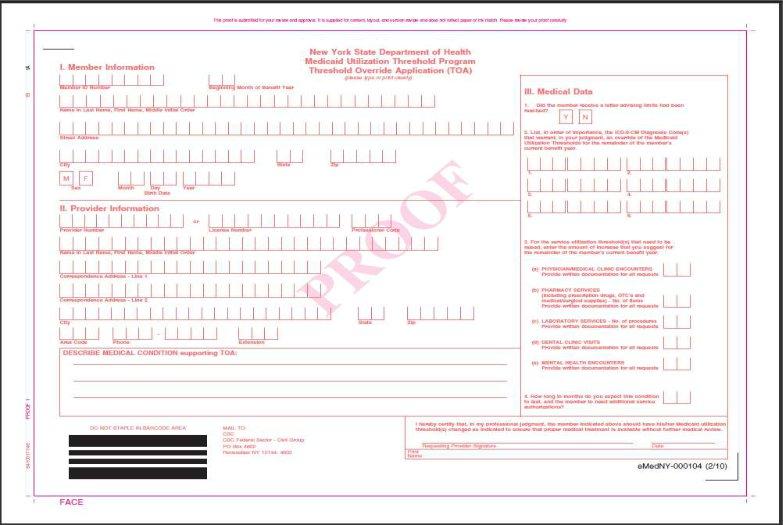
1. You have to complete the medicaid threshold override form accurately, hence be mindful when working with the parts containing all of these blank fields:
Step 3: Just after going through your filled in blanks, press "Done" and you're done and dusted! Right after registering afree trial account at FormsPal, it will be possible to download medicaid threshold override form or send it via email right off. The form will also be at your disposal in your personal account page with all your changes. Whenever you work with FormsPal, you're able to fill out documents without having to get worried about information leaks or data entries getting shared. Our secure platform makes sure that your private details are stored safely.