Our PDF editor helps make completing files effortless. It is rather straightforward to enhance the [FORMNAME] document. Keep up with these particular steps if you want to accomplish this:
Step 1: Click the "Get Form Now" button to begin.
Step 2: You're now on the document editing page. You may edit, add text, highlight particular words or phrases, put crosses or checks, and insert images.
For every single part, fill out the information asked by the software.
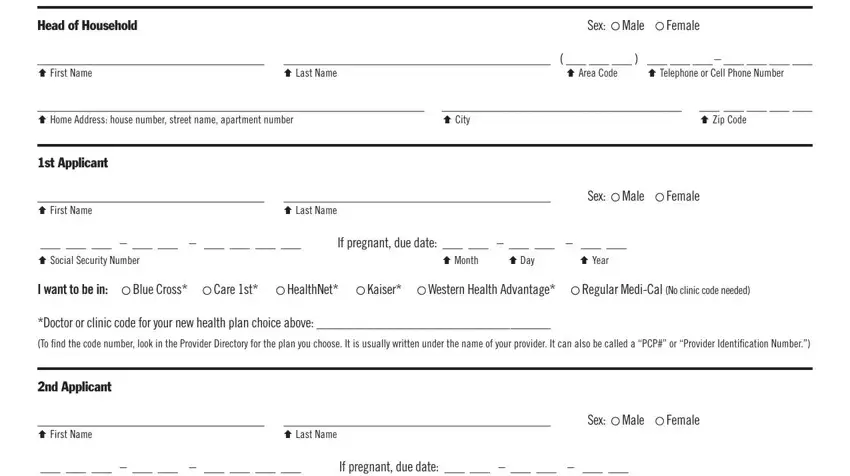
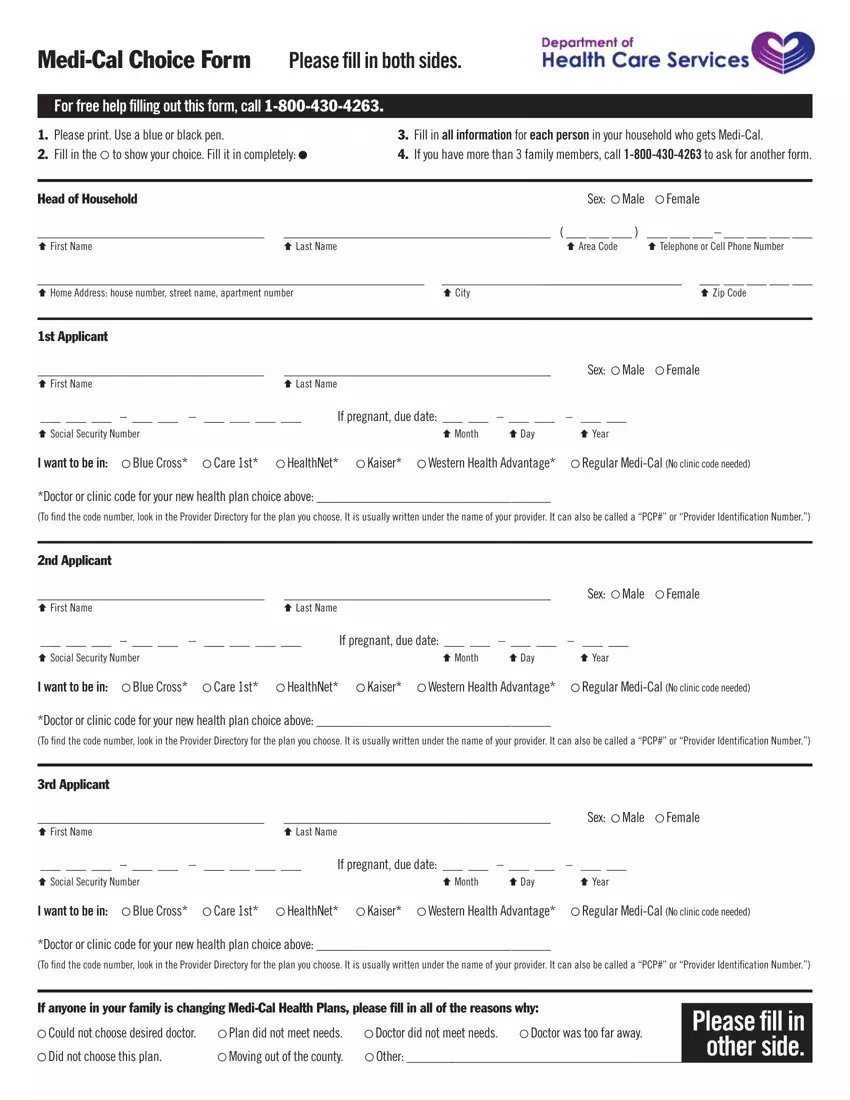
Provide the requested information in the area Ç Social Security, I want to be in, Blue Cross, Care st, HealthNet, Kaiser, Western Health Advantage, Regular MediCal No clinic code, Doctor or clinic code for your new, rd Applicant, Ç First Name, Ç Last Name, Sex, Male, and Female.
In the Head of Household, Date, Ç Signature, Ç Month Ç Day Ç Year, st Applicant if under years, Ç Signature, Ç Month Ç Day Ç Year, nd Applicant if under years, Ç Signature, Ç Month Ç Day Ç Year, rd Applicant if under years, Ç Signature, and Ç Month Ç Day Ç Year field, point out the key data.
Step 3: Hit the Done button to be sure that your finished file is available to be exported to each gadget you end up picking or mailed to an email you specify.
Step 4: Make duplicates of the form. This may protect you from possible problems. We don't view or disclose your information, hence be certain it will be secure.
