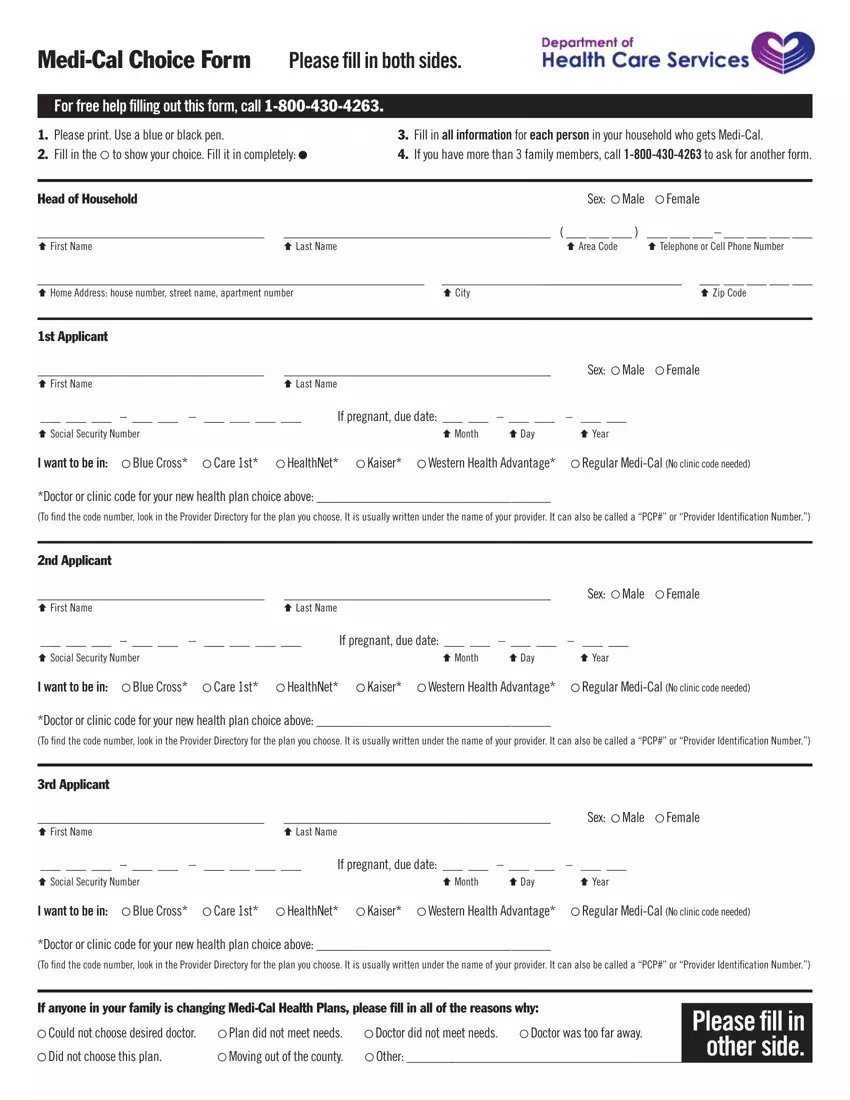
Navigating the healthcare landscape can be complex and fraught with choices that directly impact one’s health and well-being. The Medi-Cal Choice Form emerges as a crucial tool in this journey, empowering individuals and families to take control of their healthcare decisions. It requires applicants to provide comprehensive information, including personal details, for each family member receiving Medi-Cal, ensuring choices are informed and tailored to specific needs. The form accommodates choices among various healthcare plans like Blue Cross, Care 1st, HealthNet, Kaiser, and Western Health Advantage, in addition to the option of remaining with regular Medi-Cal. Specific doctor or clinic codes associated with the chosen plan must be entered, a step that highlights the importance of understanding one's healthcare provider network. The form underscores the need for meticulousness by prompting for complete filling on both sides and offers support via a free help line, reflecting an awareness of the challenges many face in making these decisions. Acknowledgment sections reinforce the gravity of choices made, informing applicants of how their information is used and introducing the concept of binding arbitration for certain choices, such as joining Kaiser. This element of the form illustrates the broader implications of selecting a healthcare plan, intertwining legal understanding with medical decision-making. The process concludes with a requirement for signatures, cementing the choices and ensuring accountability and understanding from all parties involved. The Medi-Cal Choice Form thus stands as a testament to the structured yet flexible approach required to navigate California’s healthcare system, embodying the intersection of healthcare, law, and personal choice.
| Question | Answer |
|---|---|
| Form Name | Medical Choice Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | medical choice form ca, medi cal healthcare options form, medi cal choice, medi cal choice form download |
