
When working in the online editor for PDFs by FormsPal, you can fill in or alter medical history form here. FormsPal team is committed to providing you with the best possible experience with our tool by regularly releasing new features and improvements. With all of these updates, working with our editor gets better than ever! With a few basic steps, it is possible to start your PDF editing:
Step 1: First of all, access the pdf editor by pressing the "Get Form Button" in the top section of this page.
Step 2: With our handy PDF tool, you'll be able to accomplish more than simply fill out blank fields. Express yourself and make your forms seem great with customized textual content incorporated, or tweak the original input to excellence - all that comes with the capability to insert stunning pictures and sign it off.
Completing this PDF will require attentiveness. Make certain every field is done accurately.
1. While filling out the medical history form, make sure to incorporate all of the necessary blank fields in their associated area. This will help to facilitate the work, allowing for your details to be processed swiftly and accurately.
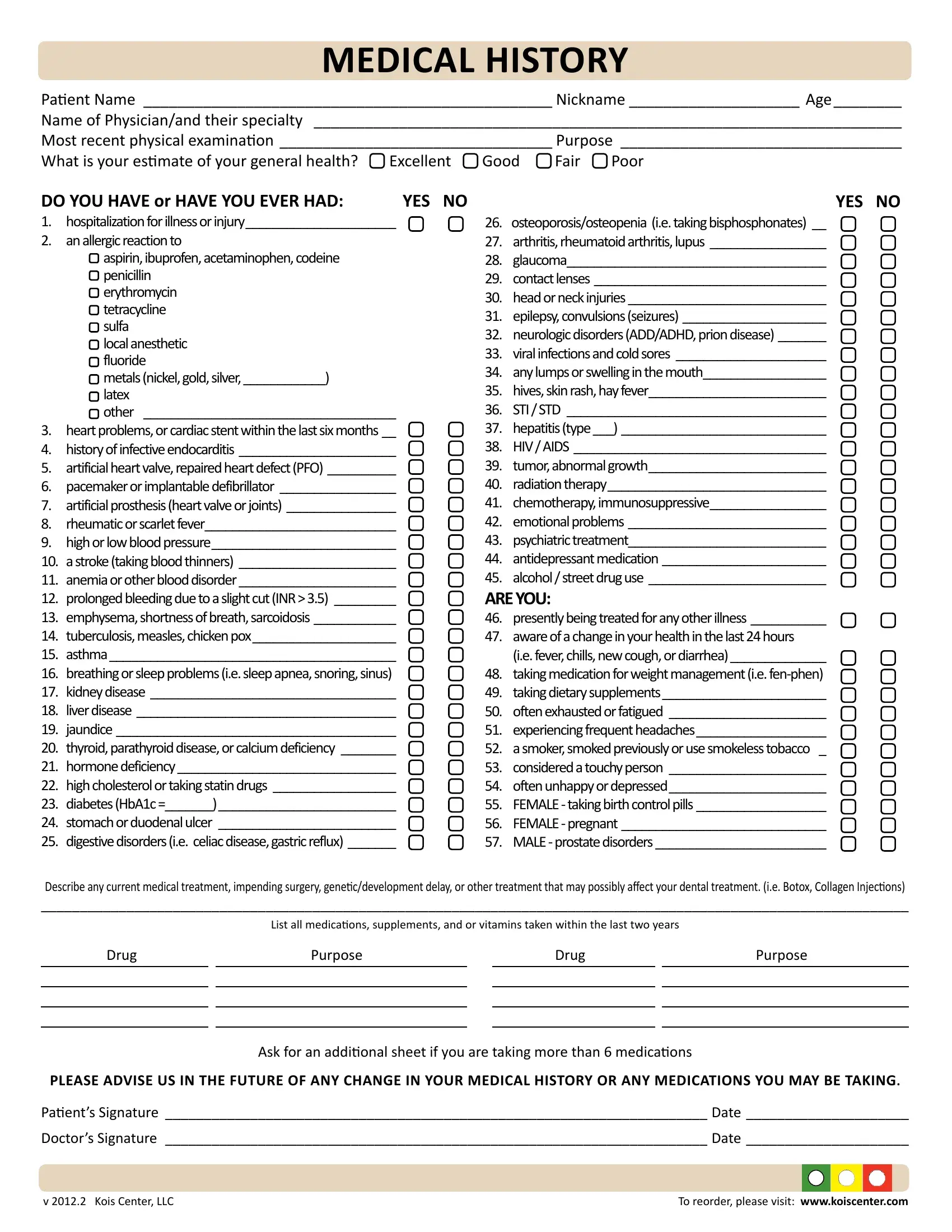
2. Now that the last array of fields is completed, you have to insert the needed particulars in DO YOU HAVE or HAVE YOU EVER HAD, osteoporosisosteopenia ie taking, Describe any current medical, and List all medicaions supplements so you can move on to the 3rd part.
Concerning DO YOU HAVE or HAVE YOU EVER HAD and List all medicaions supplements, be certain that you double-check them in this section. The two of these could be the key ones in this file.
3. Through this part, take a look at Drug, Purpose, Drug, Purpose, Ask for an addiional sheet if you, PLEASE ADVISE US IN THE FUTURE OF, Paients Signature Date Doctors, v Kois Center LLC, and To reorder please visit. All these will have to be filled in with highest attention to detail.
Step 3: Revise the details you've entered into the form fields and then hit the "Done" button. Right after setting up afree trial account with us, it will be possible to download medical history form or email it immediately. The document will also be at your disposal via your personal account with your each and every modification. FormsPal offers risk-free form completion without personal information record-keeping or sharing. Be assured that your information is safe here!