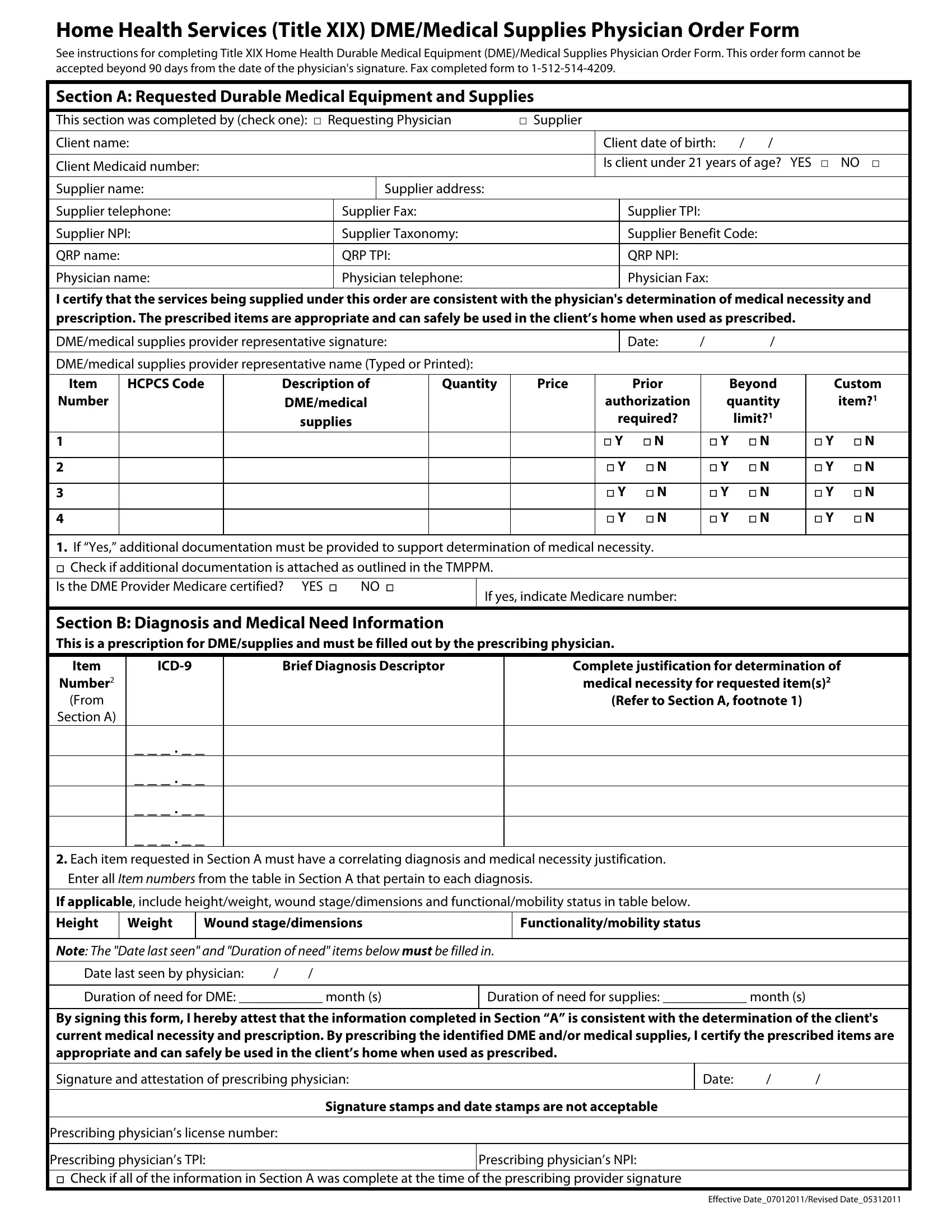
Navigating the complexities of healthcare requires understanding the tools and documents that link patient care with appropriate medical equipment and supplies. Among these, the Medical Physician Order Form stands as a pivotal document that facilitates the provision of home health services, Durable Medical Equipment (DME), and medical supplies under Title XIX. This comprehensive form serves as a bridge between the physician's assessment of medical necessity and the actual delivery of prescribed items to the patient's home, ensuring that the equipment and supplies provided are exactly what the doctor ordered to manage the patient’s health condition optimally. It outlines specific instructions for completion, emphasizing that the form be submitted within 90 days from the physician's signature to remain valid. Furthermore, it meticulously records the requested DME and supplies, client information, and crucial medical justification, all while operating within the regulatory framework of Medicaid and Medicare. The form also mandates the detailed listing of each item, including HCPCS codes, descriptions, quantities, and price, alongside a section for diagnosis and medical need information to articulate the medical rationale behind each request. By streamlining the documentation and approval process for necessary medical equipment and supplies, the form ensures that individuals receive timely and appropriate care, directly impacting their health outcomes and quality of life.
| Question | Answer |
|---|---|
| Form Name | Medical Physician Order Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | physician order form for home health, title xix medical form, doctors order form, how to xix form |
Home Health Services (Title XIX) DME/Medical Supplies Physician Order Form
See instructions for completing Title XIX Home Health Durable Medical Equipment (DME)/Medical Supplies Physician Order Form. This order form cannot be accepted beyond 90 days from the date of the physician's signature. Fax completed form to
Section A: Requested Durable Medical Equipment and Supplies
This section was completed by (check one): □ Requesting Physician |
□ Supplier |
|
|
||||
Client name: |
|
|
|
Client date of birth: |
/ |
/ |
|
|
|
|
|
|
|
||
Client Medicaid number: |
|
|
|
Is client under 21 years of age? YES □ NO □ |
|||
|
|
|
|
|
|
|
|
Supplier name: |
|
Supplier address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Supplier telephone: |
Supplier Fax: |
|
|
Supplier TPI: |
|
|
|
|
|
|
|
|
|
||
Supplier NPI: |
Supplier Taxonomy: |
|
|
Supplier Benefit Code: |
|
||
QRP name: |
QRP TPI: |
|
|
QRP NPI: |
|
|
|
|
|
|
|
|
|
|
|
Physician name: |
Physician telephone: |
|
|
Physician Fax: |
|
|
|
|
|
|
|
|
|
|
|
I certify that the services being supplied under this order are consistent with the physician's determination of medical necessity and prescription. The prescribed items are appropriate and can safely be used in the client’s home when used as prescribed.
DME/medical supplies provider representative signature: |
Date: |
/ |
/ |
DME/medical supplies provider representative name (Typed or Printed):
Item |
HCPCS Code |
Description of |
Quantity |
Price |
Prior |
Beyond |
Custom |
Number |
|
DME/medical |
|
|
authorization |
quantity |
item?1 |
|
|
supplies |
|
|
required? |
limit?1 |
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
□ Y □ N |
□ Y □ N |
□ Y □ N |
|
|
|
|
|
|
|
|
2 |
|
|
|
|
□ Y □ N |
□ Y □ N |
□ Y □ N |
|
|
|
|
|
|
|
|
3 |
|
|
|
|
□ Y □ N |
□ Y □ N |
□ Y □ N |
|
|
|
|
|
|
|
|
4 |
|
|
|
|
□ Y □ N |
□ Y □ N |
□ Y □ N |
|
|
|
|
|
|
|
|
1.If “Yes,” additional documentation must be provided to support determination of medical necessity. □ Check if additional documentation is attached as outlined in the TMPPM.
Is the DME Provider Medicare certified? YES □ NO □
Section B: Diagnosis and Medical Need Information
This is a prescription for DME/supplies and must be filled out by the prescribing physician.
Item |
Brief Diagnosis Descriptor |
Complete justification for determination of |
|
Number2 |
|
|
medical necessity for requested item(s)2 |
(From |
|
|
(Refer to Section A, footnote 1) |
Section A) |
|
|
|
_ _ _ . _ _
_ _ _ . _ _
_ _ _ . _ _
_ _ _ . _ _
2.Each item requested in Section A must have a correlating diagnosis and medical necessity justification. Enter all ITEM NUMBERS from the table in Section A that pertain to each diagnosis.
If applicable, include height/weight, wound stage/dimensions and functional/mobility status in table below.
Height
Weight
Wound stage/dimensions
Functionality/mobility status
NOTE: THE "DATE LAST SEEN" AND "DURATION OF NEED" ITEMS BELOW MUST BE FILLED IN.
Date last seen by physician: |
/ |
/ |
Duration of need for DME: ____________ month (s)
Duration of need for supplies: ____________ month (s)
By signing this form, I hereby attest that the information completed in Section “A” is consistent with the determination of the client's current medical necessity and prescription. By prescribing the identified DME and/or medical supplies, I certify the prescribed items are appropriate and can safely be used in the client’s home when used as prescribed.
Signature and attestation of prescribing physician:
Date: |
/ |
/ |
Signature stamps and date stamps are not acceptable
Prescribing physician’s license number:
Prescribing physician’s TPI: |
Prescribing physician’s NPI: |
□Check if all of the information in Section A was complete at the time of the prescribing provider signature
Effective Date_07012011/Revised Date_05312011