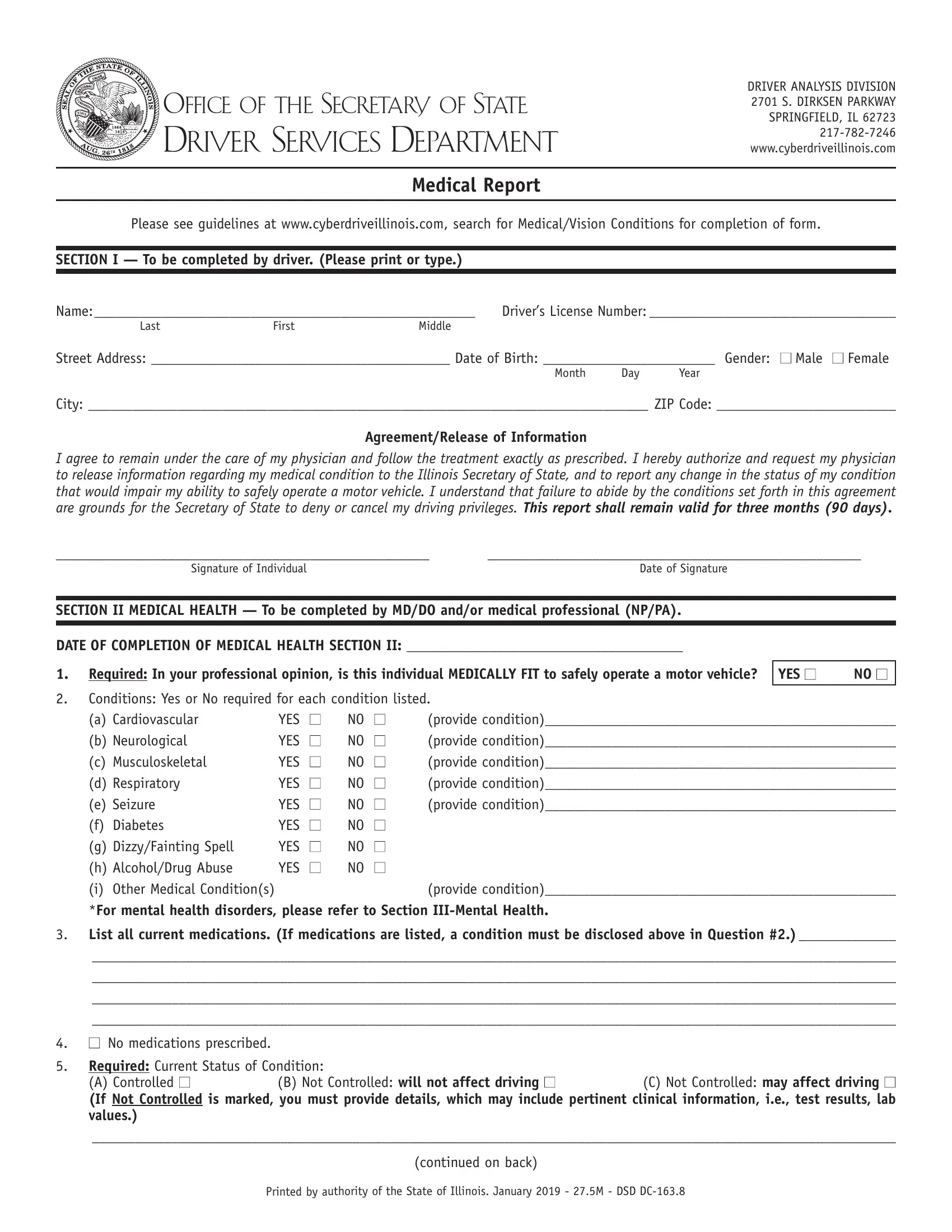
OFFICE OF THE SECRETARY OF STATE
DRIVER SERVICES DEPARTMENT
DRIVER ANALYSIS DIVISION 2701 S. DIRKSEN PARKWAY SPRINGFIELD, IL 62723 217-782-7246 www.cyberdriveillinois.com
Medical Report
Please see guidelines at www.cyberdriveillinois.com, search for Medical/Vision Conditions for completion of form.
SECTION I — To be completed by driver. (Please print or type.)
Name: ___________________________________________________ |
Driver’s License Number: _________________________________ |
Last |
First |
Middle |
|
Street Address: ________________________________________ Date of Birth: _______________________ Gender: ■ Male ■ Female
Month Day Year
City: ___________________________________________________________________________ ZIP Code: ________________________
Agreement/Release of Information
I agree to remain under the care of my physician and follow the treatment exactly as prescribed. I hereby authorize and request my physician to release information regarding my medical condition to the Illinois Secretary of State, and to report any change in the status of my condition that would impair my ability to safely operate a motor vehicle. I understand that failure to abide by the conditions set forth in this agreement are grounds for the Secretary of State to deny or cancel my driving privileges. This report shall remain valid for three months (90 days).
__________________________________________________ |
__________________________________________________ |
Signature of Individual |
Date of Signature |
SECTION II MEDICAL HEALTH — To be completed by MD/DO and/or medical professional (NP/PA).
DATE OF COMPLETION OF MEDICAL HEALTH SECTION II: _____________________________________
1.Required: In your professional opinion, is this individual MEDICALLY FIT to safely operate a motor vehicle?
2.Conditions: Yes or No required for each condition listed.
(a) Cardiovascular |
YES |
■ |
NO |
■ |
(provide condition)_______________________________________________ |
(b) Neurological |
YES |
■ |
NO |
■ |
(provide condition)_______________________________________________ |
(c) Musculoskeletal |
YES |
■ |
NO |
■ |
(provide condition)_______________________________________________ |
(d) Respiratory |
YES |
■ |
NO |
■ |
(provide condition)_______________________________________________ |
(e) Seizure |
YES |
■ |
NO |
■ |
(provide condition)_______________________________________________ |
(f) Diabetes |
YES |
■ |
NO |
■ |
|
(g) Dizzy/Fainting Spell |
YES |
■ |
NO |
■ |
|
(h) Alcohol/Drug Abuse |
YES |
■ |
NO |
■ |
|
(i) Other Medical Condition(s) |
|
|
|
|
(provide condition)_______________________________________________ |
*For mental health disorders, please refer to Section III-Mental Health.
3.List all current medications. (If medications are listed, a condition must be disclosed above in Question #2.) _____________
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
4.■ No medications prescribed.
5.Required: Current Status of Condition:
(A) Controlled ■(B) Not Controlled: will not affect driving ■(C) Not Controlled: may affect driving ■
(If Not Controlled is marked, you must provide details, which may include pertinent clinical information, i.e., test results, lab values.)
_______________________________________________________________________________________________________________
(continued on back) Printed by authority of the State of Illinois. January 2019 - 27.5M - DSD DC-163.8
PATIENT’S NAME: ________________________________________________
6.Required: In the past six months, has the driver’s ability to safely operate a motor vehicle been impaired (due to any reason) or has
driver experienced an attack of unconsciousness? |
YES ■ |
NO ■ |
Date of Attack: ___________________ |
(If YES, you must provide details, which may include pertinent clinical information.)
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
7.Date of last impaired ability to safely operate a motor vehicle or attack of unconsciousness. Date: ___________________
(You must provide details, which may include pertinent clinical information.)
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
SECTION III MENTAL HEALTH — To be completed ONLY if driver has a Mental Health Disorder marked “YES” by MD/DO and/or medical professional (NP/PA).
Mental Health Disorder: YES ■ NO ■
DATE OF COMPLETION OF MENTAL HEALTH SECTION III: _____________________________________
1.Required: In your professional opinion, is this individual MENTALLY FIT to safely operate a motor vehicle?
2.Mental Health Disorder Diagnosis/Condition(s): _____________________________________________________________________
3.List all current mental health medications. (If medications are listed, a condition must be disclosed above in Question #2.)
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
4.■ No medications prescribed.
5. (A) Controlled ■ |
(B) Not Controlled: will not affect driving ■ |
(C) Not Controlled: may affect driving ■ |
(If Not Controlled is marked, you must provide details, which may include pertinent clinical information, i.e., test results, lab values.)
_______________________________________________________________________________________________________________
SECTION IV — Additional information, special restrictions, etc.
___________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________
SECTION V — MD/DO and/or medical professional (NP/PA) — Failure to provide license information will result in return of form to the driver.
(Unacceptable Signatures: Chiropractors, Podiatrists, Residents, Fellows, Interns, RN’s, LPN’s, Co-signatures)
MEDICAL: |
|
|
|
______________________________________________________ |
_______________________________________________________ |
Provider Name (PRINTED) |
Medical Provider’s Address (PRINTED/STAMPED) |
______________________________________________________ |
( |
) |
|
_______________________________________________________ |
Professional License Number/State License Issued |
Telephone Number |
______________________________________________________ |
_______________________________________________________ |
Provider’s SIGNATURE — Date of Completion |
■ MD |
■ DO |
■ NP ■ PA Provider’s Specialty |
MENTAL: |
|
|
|
______________________________________________________ |
_______________________________________________________ |
Provider Name (PRINTED) |
Medical Provider’s Address (PRINTED/STAMPED) |
______________________________________________________ |
( |
) |
|
_______________________________________________________ |
Professional License Number/State License Issued |
Telephone Number |
______________________________________________________ |
_______________________________________________________ |
Provider’s SIGNATURE — Date of Completion |
■ MD |
■ DO |
■ NP ■ PA Provider’s Specialty |
PLEASE MAINTAIN A COPY FOR YOUR RECORDS.