The process of completing the medicare wellness exam form printable is actually effortless. Our experts made sure our PDF editor is easy to utilize and can help complete virtually any PDF without delay. Learn about several simple steps you will have to take:
Step 1: On the following webpage, press the orange "Get form now" button.
Step 2: Once you get into the medicare wellness exam form printable editing page, you will see all the actions it is possible to take with regards to your document within the top menu.
The next areas are going to make up your PDF file:
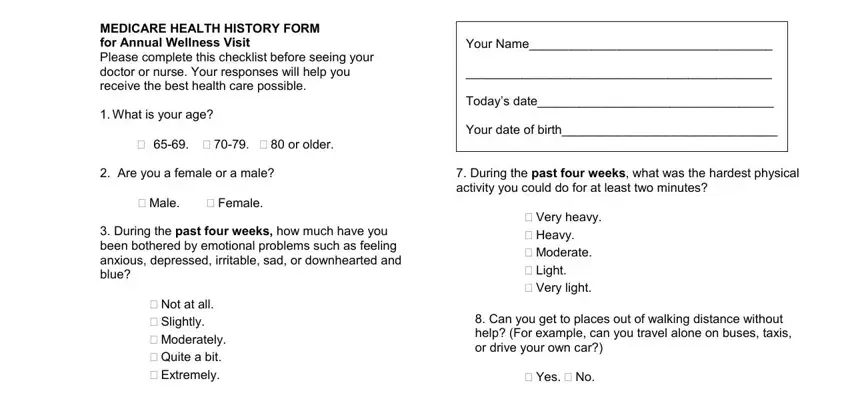
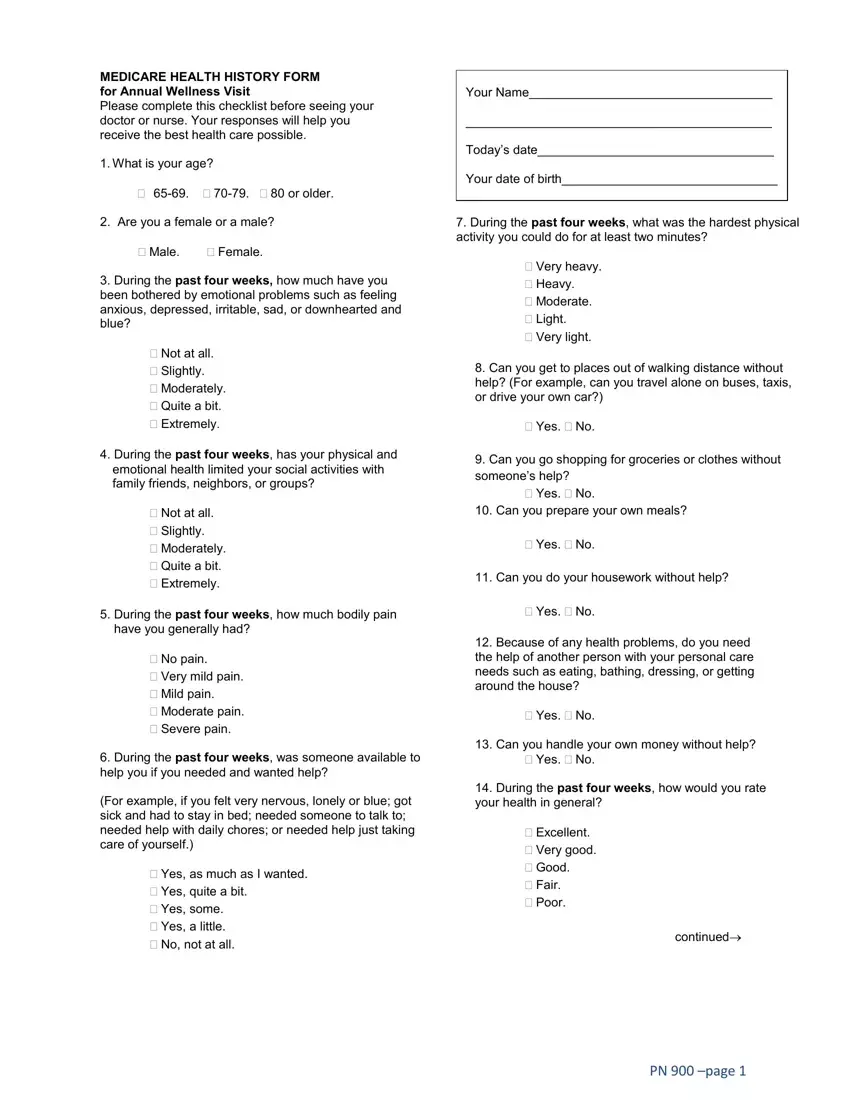
You should prepare the During the past four weeks has, Not at all Slightly Moderately, Can you go shopping for groceries, Yes No, Can you prepare your own meals, Yes No, Can you do your housework without, During the past four weeks how, Yes No, No pain Very mild pain Mild, During the past four weeks was, For example if you felt very, Yes as much as I wanted Yes, Because of any health problems do, and Yes No box with the essential information.
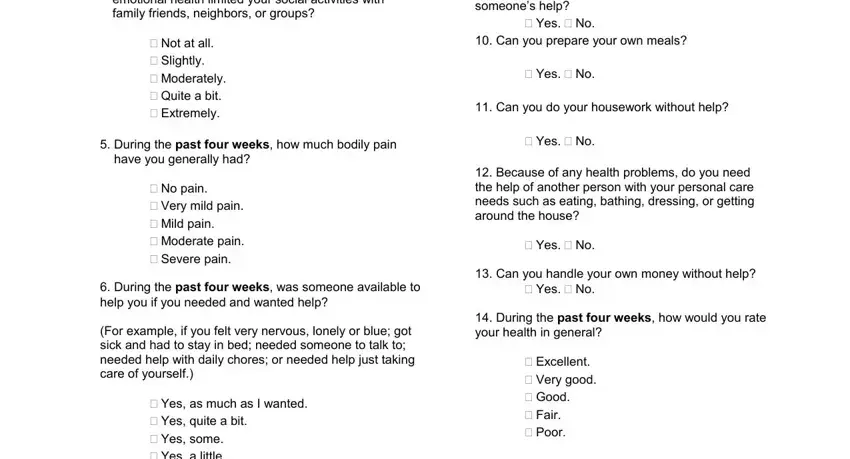
Jot down the essential data in Yes as much as I wanted Yes, continued, and PN page area.

Inside the field Patient Name, DOBTodays Date, How have things been going for, During the past four weeks how, Very well could hardly be better, or more drinks per week drinks, Are you having difficulties, Do you exercise for about, Yes often Sometimes No Not, Yes most of the time Yes some of, Do you always fasten your seat, Have you been given any, Yes usually Yes sometimes No, How often during the past four, and Hazards in your house that might, list the rights and responsibilities of the parties.
End by looking at the next areas and filling in the suitable information: m o d l e S, r e v e N, i t e m o S, n e t f, s y a w A, Falling or dizzy when standing up, Have you fallen two or more times, Yes No, Are you afraid of falling, Yes No, Are you a smoker, No Yes and I might quit Yes but, Checklist to bring to your, I do not have to take medicine I, and How confident are you that you.
Step 3: Press the Done button to be certain that your finished form may be exported to any device you end up picking or forwarded to an email you specify.
Step 4: To avoid any sort of hassles down the road, you will need to get minimally a few duplicates of your document.
