
You are able to work with cms 20027 pdf effortlessly with the help of our online PDF tool. To have our tool on the cutting edge of practicality, we aim to adopt user-oriented capabilities and improvements on a regular basis. We're at all times pleased to get suggestions - join us in reshaping how we work with PDF forms. With a few basic steps, you can begin your PDF editing:
Step 1: Click the "Get Form" button in the top area of this webpage to open our PDF tool.
Step 2: The tool lets you change the majority of PDF files in various ways. Improve it with customized text, correct what is originally in the file, and put in a signature - all readily available!
This PDF doc needs specific information; to ensure accuracy and reliability, remember to take into account the tips further on:
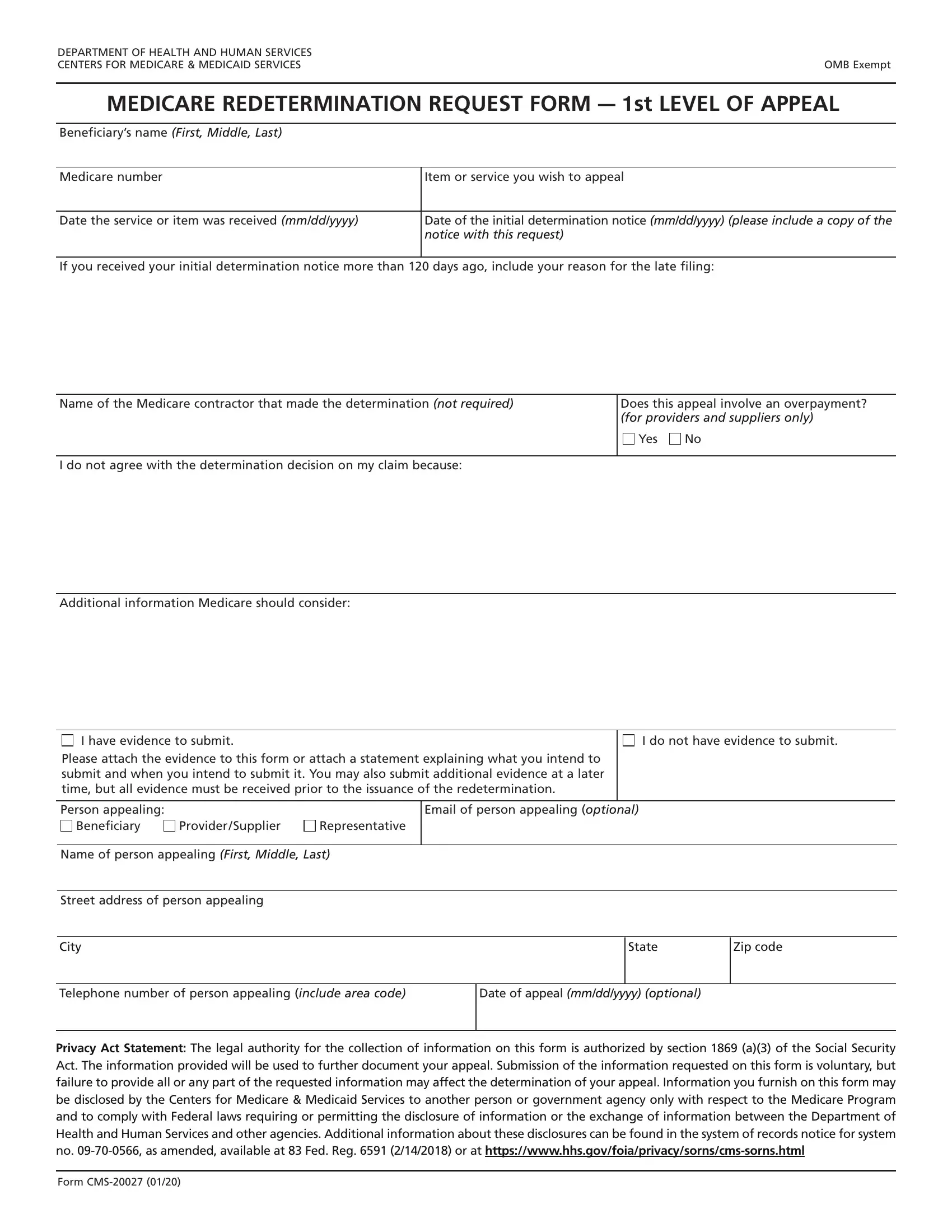
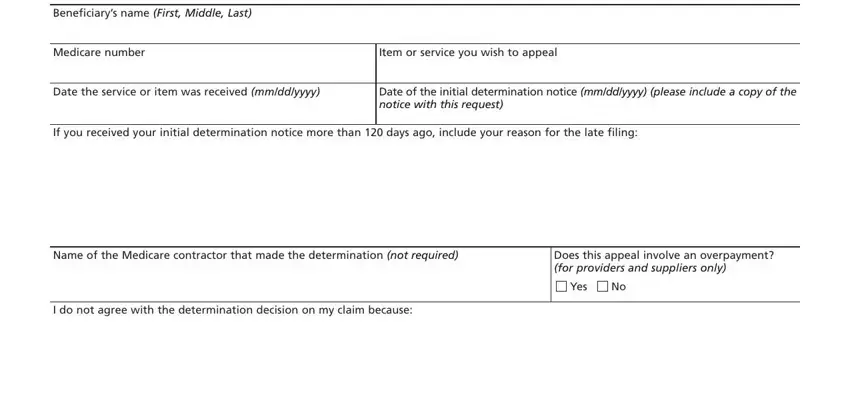
1. The cms 20027 pdf requires certain information to be typed in. Make certain the following blanks are complete:
2. Once your current task is complete, take the next step – fill out all of these fields - Additional information Medicare, I have evidence to submit, I do not have evidence to submit, Please attach the evidence to this, Person appealing, Email of person appealing optional, Beneficiary, Provider Supplier, Representative, Name of person appealing First, Street address of person appealing, City, State, Zip code, and Telephone number of person with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
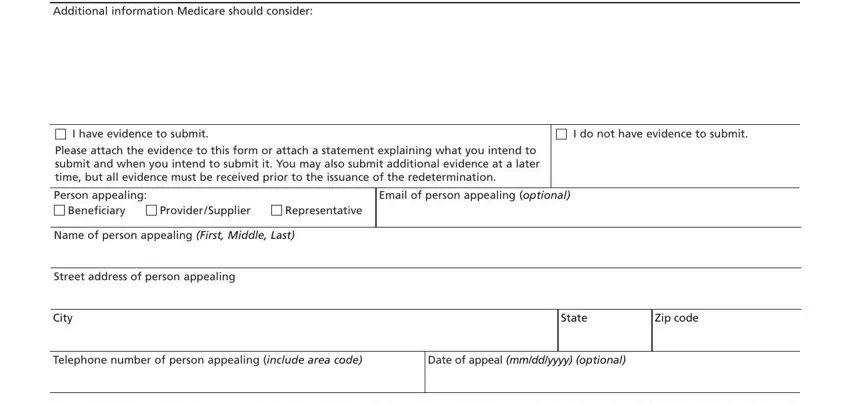
It is easy to make a mistake when completing your Zip code, and so make sure to go through it again prior to when you submit it.
Step 3: Before submitting the file, it's a good idea to ensure that blanks have been filled in as intended. Once you are satisfied with it, click “Done." After getting afree trial account at FormsPal, it will be possible to download cms 20027 pdf or email it promptly. The file will also be accessible from your personal account menu with your each edit. We don't sell or share any details that you enter while dealing with forms at FormsPal.