

Working with PDF forms online is actually super easy with this PDF tool. You can fill out dhs form mn here in a matter of minutes. Our tool is consistently developing to provide the best user experience attainable, and that's thanks to our resolve for continual improvement and listening closely to user opinions. This is what you will want to do to begin:
Step 1: Click on the orange "Get Form" button above. It will open up our tool so that you could start filling in your form.
Step 2: The tool lets you work with PDF documents in various ways. Enhance it with customized text, correct existing content, and put in a signature - all within several mouse clicks!
This document will need some specific details; to ensure consistency, make sure you bear in mind the tips down below:
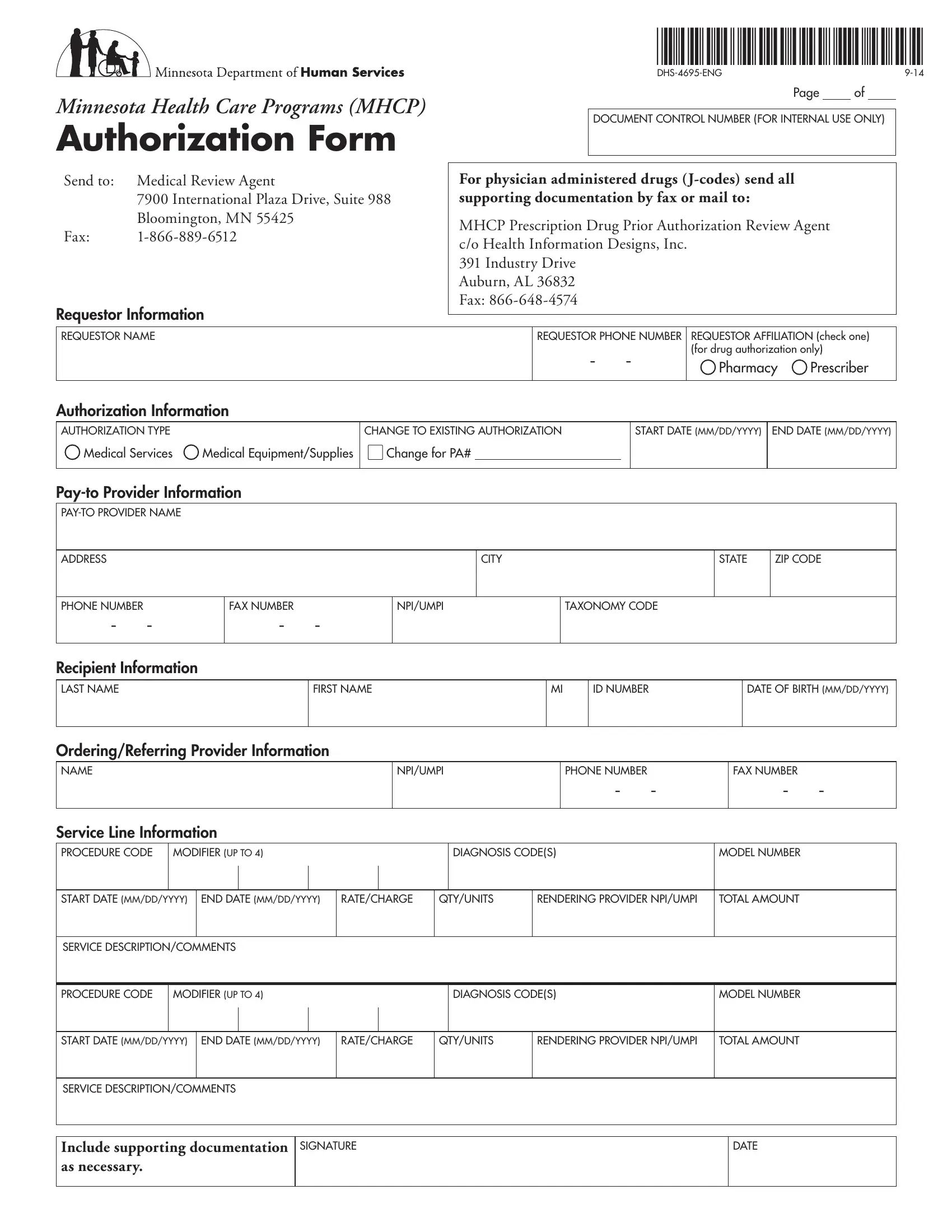
1. Before anything else, when completing the dhs form mn, start in the section that contains the next fields:
2. Immediately after this selection of blanks is completed, go to enter the suitable details in these: ADDRESS, CITY, STATE, ZIP CODE, PHONE NUMBER, FAX NUMBER, NPIUMPI, TAXONOMY CODE, Recipient Information LAST NAME, FIRST NAME, ID NUMBER, DATE OF BIRTH MMDDYYYY, OrderingReferring Provider, NPIUMPI, and PHONE NUMBER.
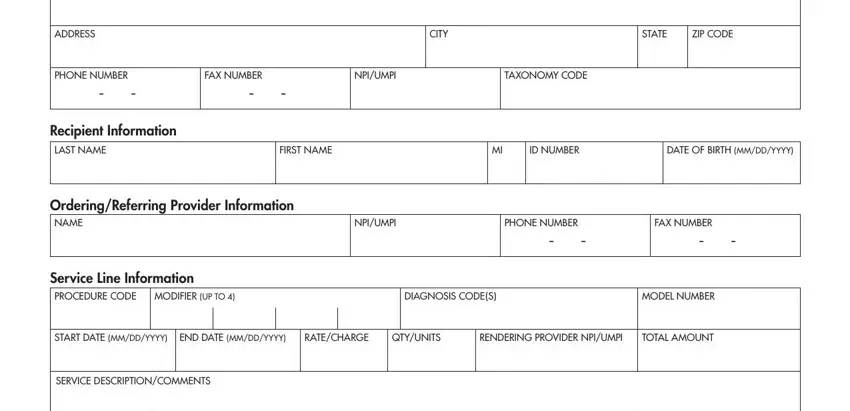
3. The following segment focuses on PROCEDURE CODE, MODIFIER UP TO, DIAGNOSIS CODES, MODEL NUMBER, START DATE MMDDYYYY, END DATE MMDDYYYY, RATECHARGE, QTYUNITS, RENDERING PROVIDER NPIUMPI, TOTAL AMOUNT, SERVICE DESCRIPTIONCOMMENTS, Include supporting documentation, SIGNATURE, and DATE - fill in every one of these blank fields.
4. To go forward, the following part will require filling out a few blanks. These comprise of For more than two services or line, Page, Recipient Information LAST NAME, Service Line Information PROCEDURE, MODIFIER UP TO, FIRST NAME, ID NUMBER, DATE OF BIRTH MMDDYYYY, DIAGNOSIS CODES, MODEL NUMBER, START DATE MMDDYYYY, END DATE MMDDYYYY, RATECHARGE, QTYUNITS, and RENDERING PROVIDER NPIUMPI, which you'll find vital to going forward with this particular PDF.
5. Now, the following last section is what you will have to wrap up prior to closing the PDF. The fields in this instance include the next: START DATE MMDDYYYY, END DATE MMDDYYYY, RATECHARGE, QTYUNITS, RENDERING PROVIDER NPIUMPI, TOTAL AMOUNT, SERVICE DESCRIPTIONCOMMENTS, PROCEDURE CODE, MODIFIER UP TO, DIAGNOSIS CODES, MODEL NUMBER, START DATE MMDDYYYY, END DATE MMDDYYYY, RATECHARGE, and QTYUNITS.
It's simple to make a mistake when completing your RATECHARGE, thus ensure that you look again before you'll finalize the form.
Step 3: Right after you've reviewed the details in the file's blanks, simply click "Done" to complete your FormsPal process. Right after starting a7-day free trial account here, you will be able to download dhs form mn or email it promptly. The document will also be accessible through your personal account with your every change. FormsPal provides safe form editing devoid of personal data recording or any sort of sharing. Be assured that your details are secure with us!