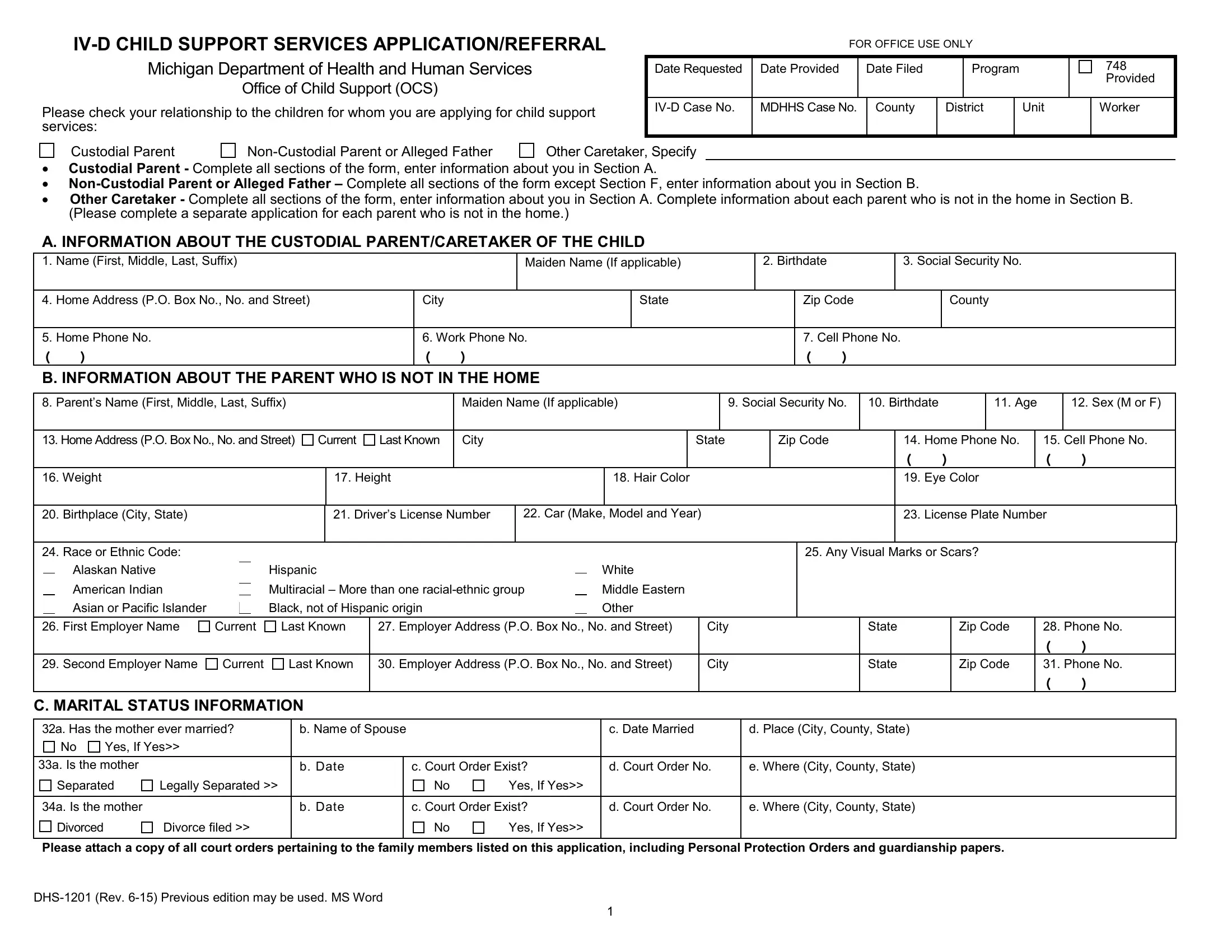
The Mi Child Support Services form, formally recognized as the IV-D CHILD SUPPORT SERVICES APPLICATION/REFERRAL, is a comprehensive document used by the Michigan Department of Health and Human Services Office of Child Support (OCS) to facilitate the application or referral for child support services within Michigan. This form is meticulously structured to collect detailed information about the custodial parent or caretaker, the non-custodial parent or alleged father, and any other relevant caretakers, including their personal, employment, and contact information. It ensures the efficient processing and management of child support cases by gathering essential data such as the child(ren)'s health care coverage, the marital status of the parents, and specific directives for handling overpayments or erroneous disbursements through the Michigan State Disbursement Unit (MiSDU). Additionally, the form outlines the legal requirements and expectations from applicants, including acknowledgements regarding the voluntary provision of social security numbers as mandated by the Social Security Act for the purpose of paternity establishment and the enforcement of child support obligations. Applicants are also informed about the implications of not providing information, which may affect their eligibility for certain benefits. This form acts as a critical liaison between custodial parents, caretakers, and the OCS, ensuring that all parties are informed about their rights and responsibilities in the child support process, and underscores Michigan's efforts to support the welfare of children through proper financial support mechanisms.
| Question | Answer |
|---|---|
| Form Name | Mi Child Support Services Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | how to mi child support services, michigan form support, mi child support, child services application |