By following these steps, you will have properly completed the Minnesota Accident Report Form, providing valuable data that assist in legal proceedings and insurance matters.
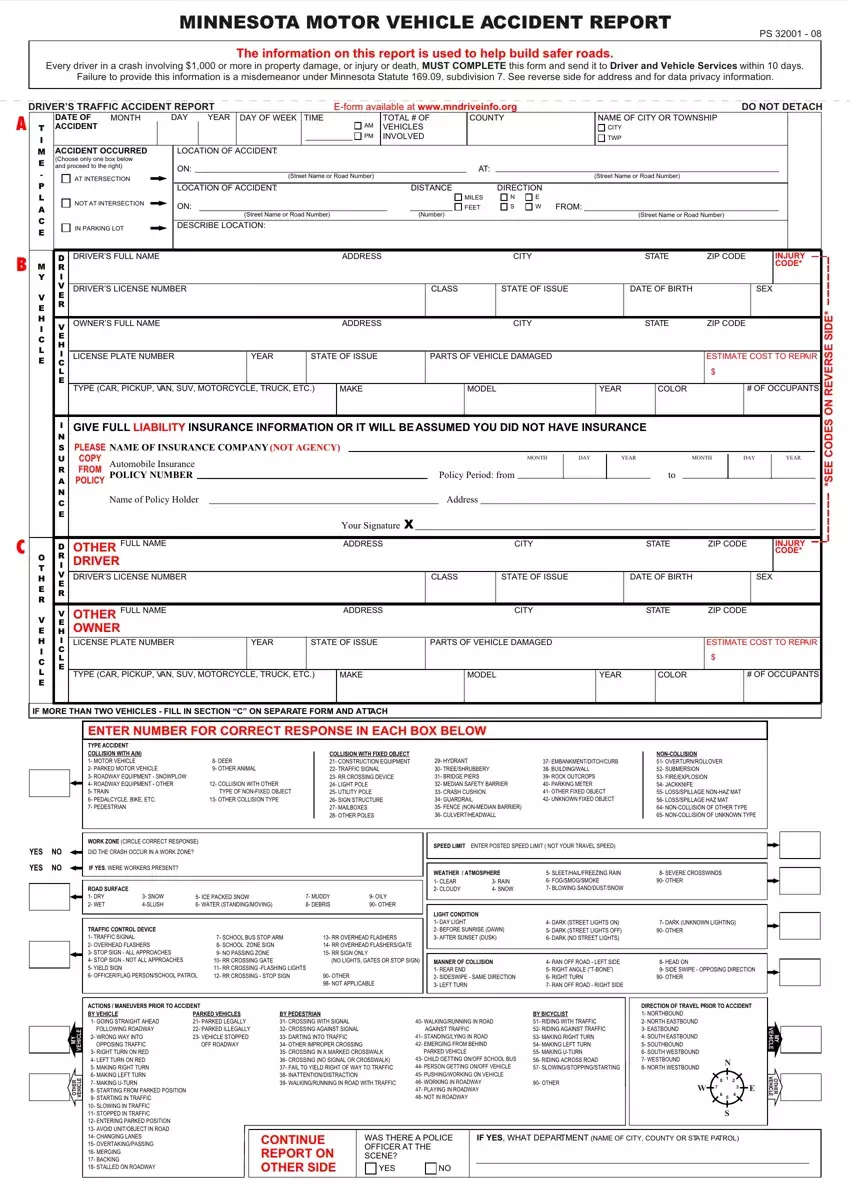
1. Provide Accident Details
Begin by documenting the specifics of the accident, including the exact date, time, and location. Ensure you describe whether the incident occurred at an intersection, in a parking lot, or on a specific section of the road.
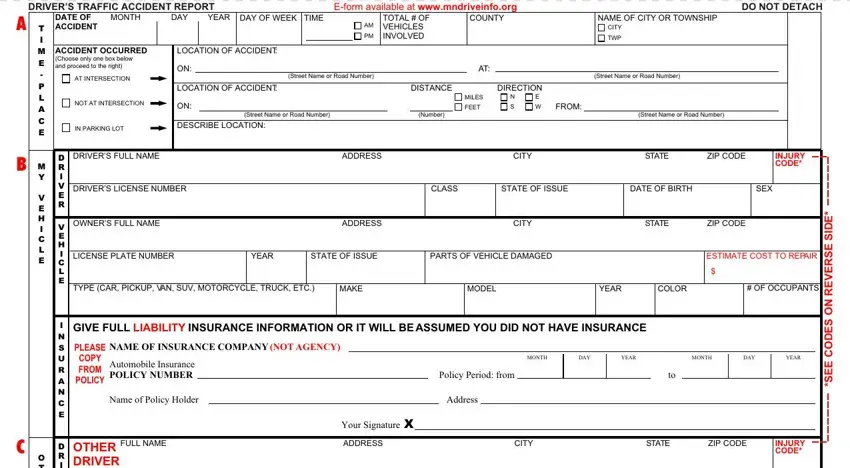
2. Detail Vehicle Information
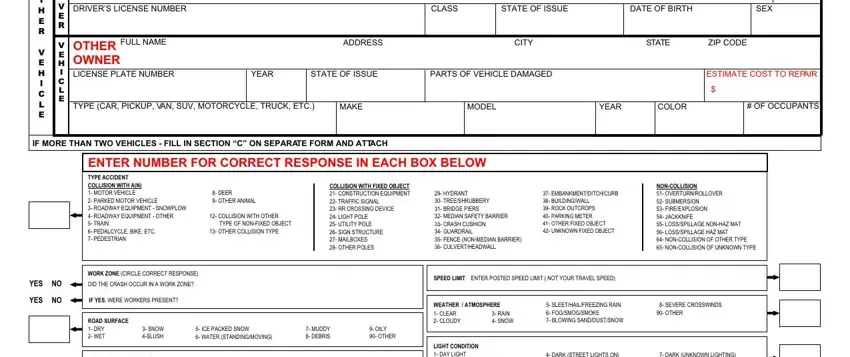
Enter all pertinent information regarding your vehicle, such as make, model, year, license plate number, and vehicle identification number (VIN). Repeat this process for the other vehicle(s) involved if applicable.
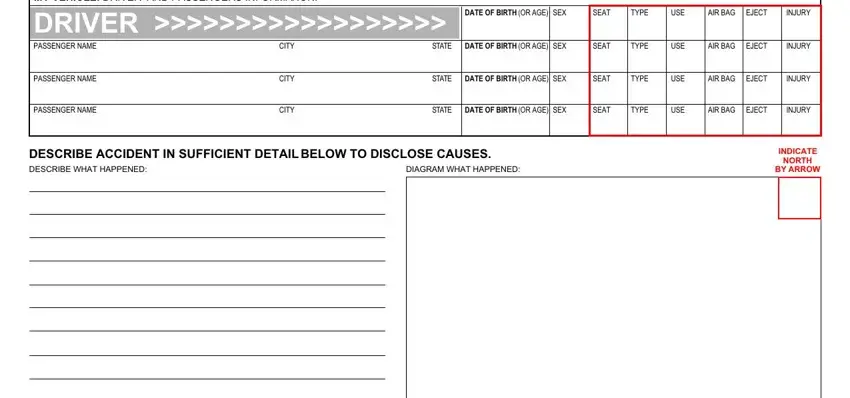
3. Record Driver Information
For each driver involved, include full name, date of birth, driver’s license number, and contact details.
4. Accident Diagram
Provide a diagram of the accident. Illustrate the positions and movements of all vehicles involved, indicating the direction each was traveling and where impacts occurred.
5. Describe the Accident
In your own words, give a detailed description of how the accident happened. Include any contributing factors like road conditions, weather, and drivers' actions leading to the accident.
6. List Damages and Injuries
Document all damages to the vehicles and other property, along with an estimated repair cost. Also, record details of any injuries sustained by drivers, passengers, or pedestrians.
7. Include Insurance Information
Fill out the insurance information for all parties involved, including the insurance company name, policy number, and the policyholder's name.
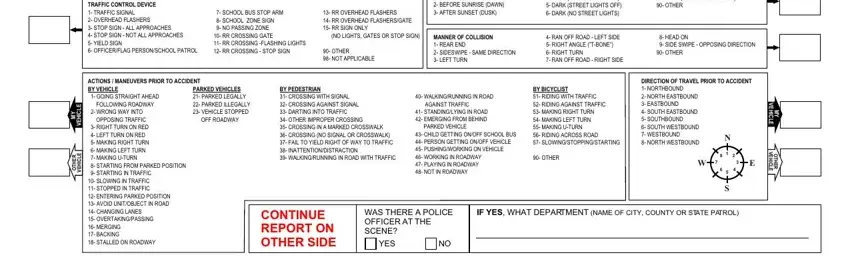
8. Traffic and Environmental Conditions
Note the traffic and environmental conditions during the accident, such as lighting, weather, and road surface conditions.
9. Compliance with Traffic Laws
Indicate any traffic laws that were violated and that contributed to the accident. This includes speeding, failure to yield, running a red light, etc.
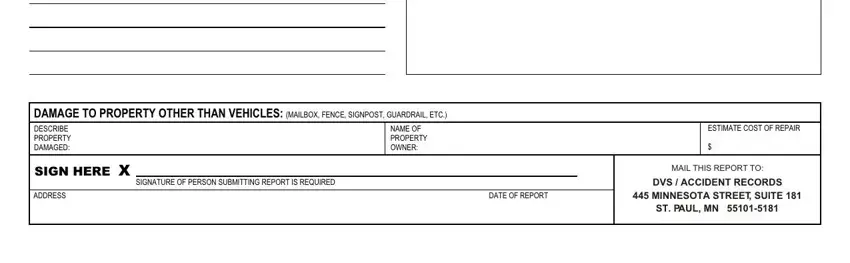
10. Final Review and Signature
Review the entire form to ensure all information is accurate and complete. Sign and date the form to verify the authenticity of the provided information.
