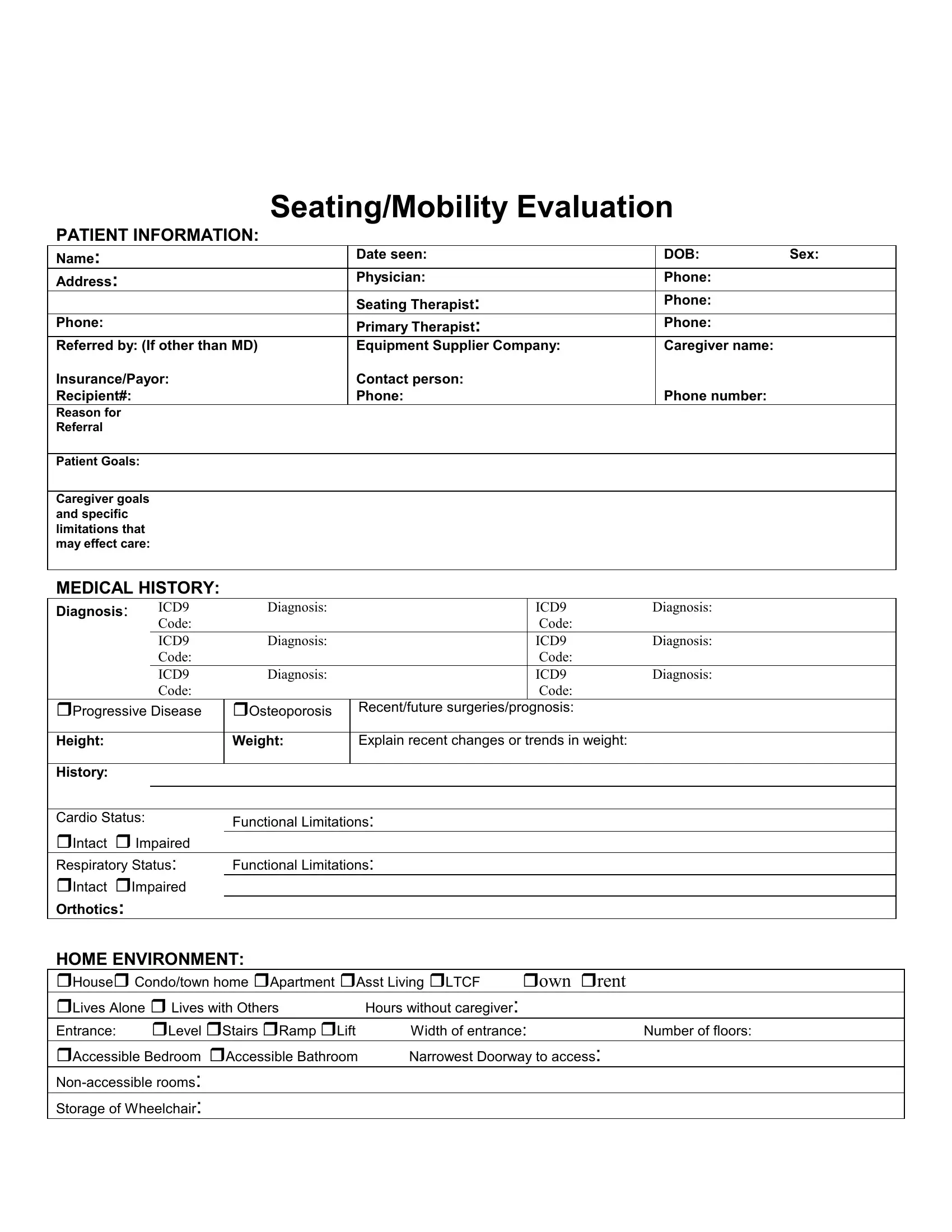
Embarking on the journey of obtaining or upgrading mobility aids involves a comprehensive process that begins with filling out the Mobility Evaluation form. This form is a detailed document that captures a wide range of essential information, starting with the basic patient information such as name, date of birth, address, and extending to intricate details concerning the patient's medical history, diagnosis codes, and information about the patient's current seating and mobility arrangements. Importantly, it dives into the patient's goals, caregiver’s expectations, and specific limitations that may influence care, thereby setting the stage for a tailored approach to mobility solutions. Moreover, the form evaluates the patient's home and community environment, their transportation needs, and their daily living activities, to ensure that any equipment recommended will enhance their quality of life. The patient’s functional and sensory processing skills are assessed to identify any areas that might affect the safe operation of a wheelchair. The evaluation also looks into the patient's communication abilities, sensation and skin integrity issues, and their current seating and mobility systems to determine the necessity for adjustments or new equipment. The form's comprehensive nature requires input from various professionals, including physicians, therapists, and equipment suppliers, underscoring the multidisciplinary approach needed for effective mobility aid provision. Thus, the Mobility Evaluation form serves as a crucial tool in mapping out an individual's specific needs and preferences, paving the way for enhanced mobility and independence.
| Question | Answer |
|---|---|
| Form Name | Mobility Evaluation Form |
| Form Length | 12 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min |
| Other names | mobility evaluation form pdf, mobility evaluation form sample, seating justification make, durable medical equipment mobility evaluation form |
