The MSC Medical Summary form serves as a crucial document within the Military Sealift Fleet Support Command, a pivotal component of ensuring the health and fitness of maritime crew members essential for the safe operation of ships. Located at 1283 Tow Way Drive in Norfolk, Virginia, this command oversees the application of rigorous health standards necessitated by the challenging seafaring environment. Crew members are exposed to numerous hazards and must maintain a level of physical fitness that allows them to operate emergency equipment, handle intensive labor tasks, and adapt to extreme conditions. This form, or an attached comprehensive report, provides a detailed assessment of a mariner's health, covering medical history, significant findings, laboratory results, and diagnoses. It emphasizes the importance of addressing potential medical issues that could affect a crew member's ability to perform duties, including the handling of fire and damage control equipment, navigating the physical challenges of a ship, and the capability to carry significant weight. Additionally, it outlines the requirements for medical professionals to include treatment plans, prognoses, limitations, and follow-up recommendations, taking into account the unique conditions of sea voyages that can last several months. This assessment is vital not only for the individual's well-being but also for the collective safety and efficiency of ship operations. Mariner's consent for the release of medical information signifies the collaborative approach to health management between individuals and the command's medical department, ensuring readiness and preventive care in the maritime setting.
| Question | Answer |
|---|---|
| Form Name | MSC Medical Summary Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 28 |
| Avg. time to fill out | 6 min 10 sec |
| Other names | military sealift form, msc medical summary, summary sealift command, medical summary form |
COMMANDER
MILITARY SEALIFT FLEET SUPPORT COMMAND
Medical Department (CODE: NO2M)
1283 Tow Way Drive
Norfolk, VA
VOICE: |
FAX: |
(757) |
(757) 443- 5767 |
________________________________________________________________________________________________
Mariner Name / last 4 SSN |
Current Assignment |
MEDICAL SUMMARY FORM
(ALTERNATIVELY, A WRITTEN REPORT THAT ADDRESSES BELOW ELEMENTS MAY BE ATTACHED)
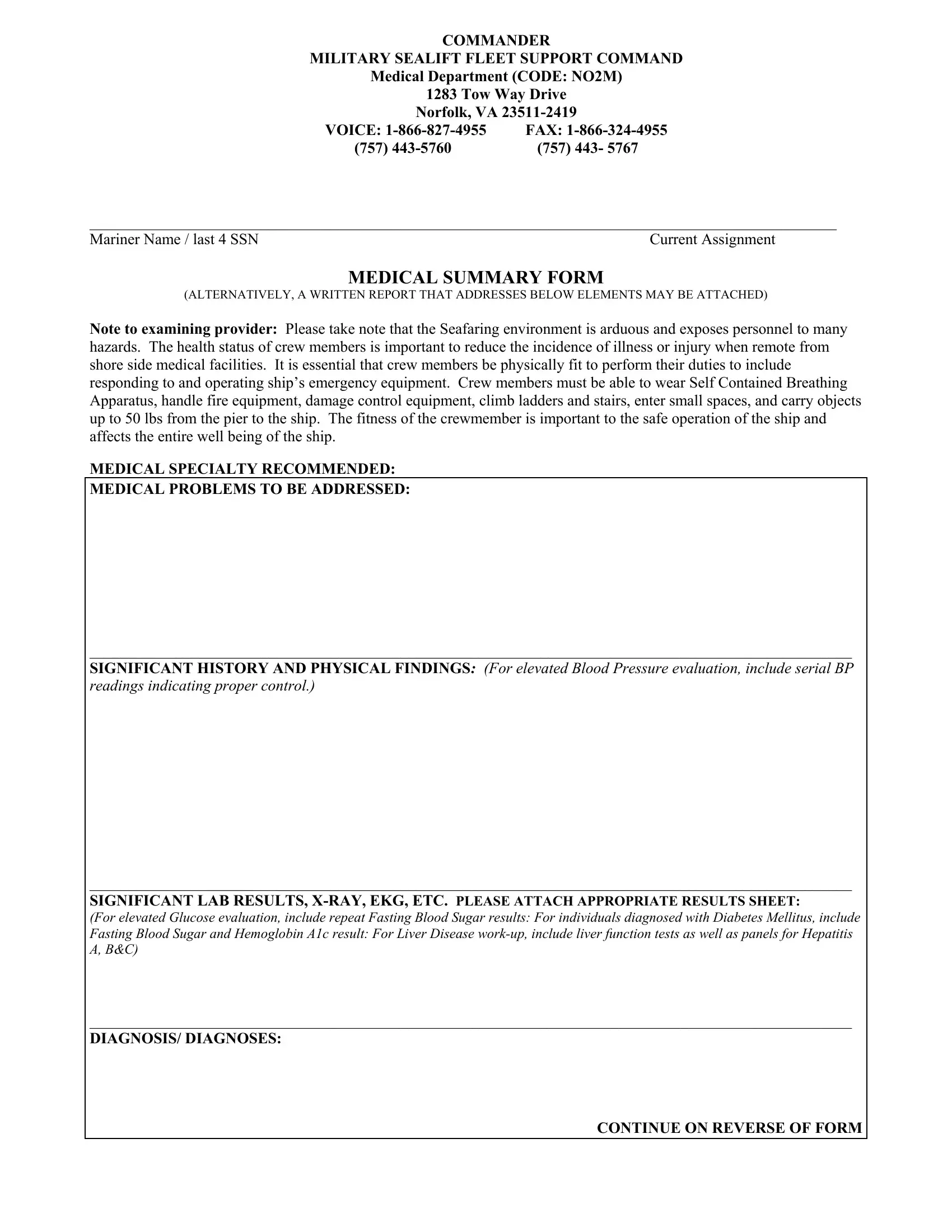
Note to examining provider: Please take note that the Seafaring environment is arduous and exposes personnel to many hazards. The health status of crew members is important to reduce the incidence of illness or injury when remote from shore side medical facilities. It is essential that crew members be physically fit to perform their duties to include responding to and operating ship’s emergency equipment. Crew members must be able to wear Self Contained Breathing Apparatus, handle fire equipment, damage control equipment, climb ladders and stairs, enter small spaces, and carry objects up to 50 lbs from the pier to the ship. The fitness of the crewmember is important to the safe operation of the ship and affects the entire well being of the ship.
MEDICAL SPECIALTY RECOMMENDED:
MEDICAL PROBLEMS TO BE ADDRESSED:
__________________________________________________________________________________________________
SIGNIFICANT HISTORY AND PHYSICAL FINDINGS: (For elevated Blood Pressure evaluation, include serial BP readings indicating proper control.)
__________________________________________________________________________________________________
SIGNIFICANT LAB RESULTS,
(For elevated Glucose evaluation, include repeat Fasting Blood Sugar results: For individuals diagnosed with Diabetes Mellitus, include
Fasting Blood Sugar and Hemoglobin A1c result: For Liver Disease
__________________________________________________________________________________________________
DIAGNOSIS/ DIAGNOSES:
CONTINUE ON REVERSE OF FORM
Page 2: Patient’s name/ssn:__________________________________
TREATMENT RECEIVED (List all medications, physical therapy, etc.)
__________________________________________________________________________________________________
PROGNOSIS / LIMITATIONS / RECOMMENDATIONS FOR FOLLOW UP. Please note that this Mariner is subject to long
Periods of
_________________________________________________________________________________________________________________________
AUTHORITY TO RELEASE PRIVILEGED MEDICAL INFORMATION: I hereby authorized release to the Medical Officer, Military Sealift Fleet Support Command, privileged medical correspondence and records in my case.
___________________________________________ |
__________________ |
Mariner’s signature |
Date |
Your current phone number where you can be reached: ______________________________________
__________________________________________________________________________________________________
____________________________________________ |
______________________________________ |
Physician’s Name |
Physician’s Signature |
_____________________________________________ |
_____________________________________ |
Please indicate your specialty and accreditation |
Date signed by Physician |
ADDRESS:TELEPHONE
()
Medical Summary Form ( (Revised 1/18/07)