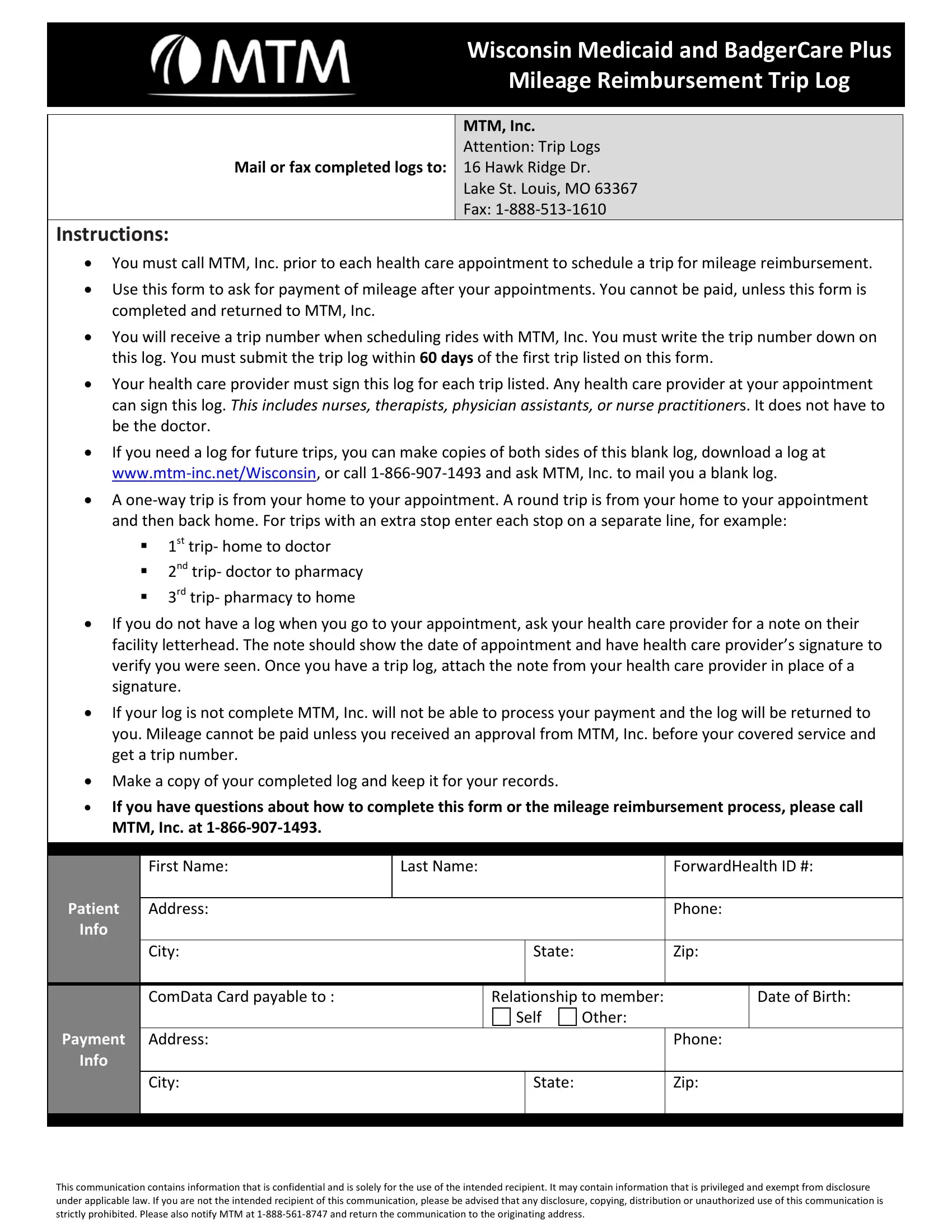
Access to healthcare is a fundamental need for all community members, especially for those enrolled in Wisconsin Medicaid and BadgerCare Plus programs. One critical aspect of this access involves transportation to and from healthcare appointments, a need that the state recognizes and addresses through the Mileage Reimbursement Trip Log administered by MTM, Inc. This process requires beneficiaries to proactively contact MTM, Inc. to schedule their trips prior to their appointments to qualify for mileage reimbursement. The form itself serves as a detailed record of each trip, including information such as the trip number, dates, types of trips (one-way or round), and healthcare provider endorsements for each visit. It's important for participants to understand that reimbursement is contingent upon the completeness of this log, obtaining a trip number in advance, and submitting the form within the stipulated 60-day period after the first trip listed. Moreover, health care providers' validation of each visit on the log underscores the importance of coordination between patients and providers. This process emphasizes proactive planning, timely submission of documentation, and adherence to guidelines to ensure that participants receive the mileage reimbursement to which they are entitled. As beneficiaries navigate their healthcare journeys, understanding and utilizing the Mileage Reimbursement Trip Log becomes an essential component of accessing necessary healthcare services while managing associated transportation costs.
| Question | Answer |
|---|---|
| Form Name | Mtm Badgercare Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | mtm wisconsin trip log, mtm wisconsin medicaid, mtm mileage reimbursement, mtm mileage reimbursement trip log |