Instructions:
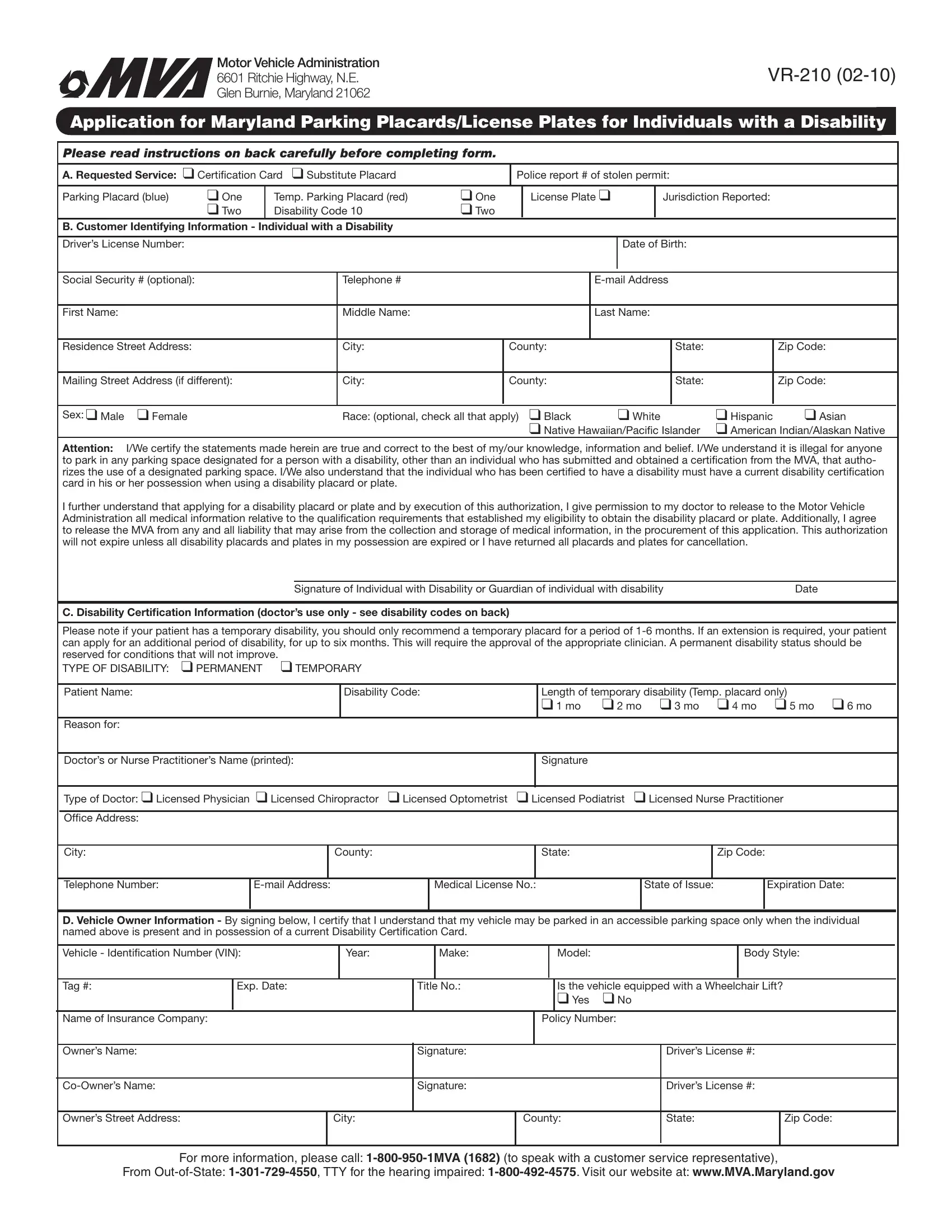
Form Purpose: An individual with a disability may use this form to request placards and/or license plates that will allow a vehicle in which he/she is
riding to park in an accessible parking space. Two types of placards are available: Temporary Placards (red), which are valid for a period of up to 6 months; and Parking Placards (blue), which are valid for four years. An applicant may request both a parking placard and disability license plates at the same time. See the Form Completion Instructions below.
Fee Information:
There is not a fee for the placard(s). A request for a disability plate requires the assessment of a substitute/replacement tag fee. Please submit your completed application along with the appropriate $20.00 fee. If requesting a disability plate and it’s time to renew your vehicle registration, the registration renewal fee is also required.
Form Completion Instructions:
Section A – Requested Service(s)
Please check the boxes, as appropriate. An individual with a disability may apply for any combination of placards and license plates, not to exceed two in number by choosing one of the following options:
• One disability placard; or |
• One disability plate; or |
• Two disability placards; or |
• One disability placard and one disability plate. |
Note: The vehicle owner must be the individual with a disability in order to qualify for issuance of a disability plate. If the individual with the disability
is not the owner or co-owner, you must apply for a disability placard.
Parking Placard (blue) - Complete Sections B and C. A doctor or licensed nurse practitioner must complete Section C (see Note below). Temporary Parking Placard (red) - Complete Sections B and C. A doctor or licensed nurse practitioner must complete Section C (see Note below). License Plates - Complete Sections B, C and D. A doctor or licensed nurse practitioner must complete Section C. You may only request a disability
plate if the vehicle is titled in the name of the individual with a disability.
Transporters of an Individual with a disability may park in designated disability parking spaces by using the individual with disabilities parking plac- ard. Transporters of an individual with a disability may not obtain a disability plate.
Note:
•A doctor’s certiication may not be required if the individual has a disability that meets the deinition of code 6 or V.
•For a replacement placard, only complete Sections A and B. For replacement plates, complete Sections A, B and D.
•A request for a replacement disability placard or plate will require you to submit a police report number and identify the jurisdiction reported.
•For temporary placards, Disability Code 10 is to be used.
Permanent Disability Codes 1-9
1. Has lung disease to such an extent that forced (respiratory) expira- |
8. Has a permanent disability, that adversely impacts the ambulatory |
tory volume for one second, when measured by spirometry, is less |
ability of the applicant and which is so severe that the person would |
than one liter, or arterial oxygen tension (p02) is less than 60 mm/hg |
endure a hardship or be subject to a risk of injury if the privileges |
on room air at rest. |
accorded a person for whom a vehicle is specially registered were |
denied.
2.Has cardiovascular disease limitations classiied in severity as Class
|
|
III or Class IV according to standards set by the American Heart |
|
9. Has a permanent impairment of both eyes so that: 1) The central |
|
|
Association. |
|
vision acuity is 20/200 or less in the better eye, with corrective |
|
|
|
|
glasses, or 2) There is a ield defect in which the peripheral ield has |
|
|
|
|
contracted to such an extent that the widest diameter of visual ield |
|
|
Is unable to walk 200 feet without stopping to rest. |
|
3. |
|
subtends an angular distance no greater than 20 degrees in the better |
|
|
|
|
eye. (See Note C) |
|
|
|
|
|
|
|
|
|
|
4. |
Is unable to walk 200 feet without the use of, or the assistance from, |
|
10. Temporary Placard (Red) requested |
|
|
a brace, cane, crutch, another person, prosthetic device, or other |
|
Disability is not permanent but would substantially impair the person’s |
|
|
assistance device. |
|
mobility or limit or impair the person’s ability to walk for at least three |
|
|
|
|
weeks, and is so severe that the person would endure a hardship or |
|
|
Requires a wheelchair for mobility. |
|
5. |
|
be subject to risk of injury if the Temporary Permit was denied. |
|
|
|
|
6. |
Has lost an arm, hand, foot, or leg. (See Note D) |
|
V. (Reserved for use by veterans with 100% disability) The Veterans |
|
|
|
|
Administration has certiied by letter that the applicant has a 100% |
7. |
Has lost the use of an arm, hand, foot or leg. |
|
|
service connected disability. |
Notes:
A.A licensed physician or licensed nurse practitioner may certify all qualifying conditions listed.
B.A licensed chiropractor or podiatrist may certify disability codes 3 through 8 and 10.
C.A licensed optometrist may certify only qualifying conditions regarding vision.
D.The person with a disability may self-certify the conditions listed under Disability Code 6 by appearing in person with proper identiication. In this situation, only the disabled person’s name and Disability Code must be recorded. If, however, a doctor certiies the loss of a limb, the doctor must complete all of Section C.
Visit your local MVA full service office or mail your application with the appropriate fees to the
Motor Vehicle Administration • 6601 Ritchie Highway, N.E., Glen Burnie, Maryland 21062. Attn: Disability Unit
Apply to...Apply to register to vote with your driver’s license transaction. For details ask your customer service representative.