The NAVMED 6120/4 form, integral to the U.S. military's healthcare system, is a comprehensive document that plays a pivotal role in ensuring service members maintain optimum health for both deployment readiness and their overall well-being. This form facilitates the Periodic Health Assessment (PHA), a routine evaluation engrained in military protocols aimed at reviewing, assessing, and addressing the health status and risk factors present in military personnel. It meticulously accounts for various health parameters including height, weight, BMI, and vital signs, among others. The form delves into subjective details provided by the individual, such as allergies, chronic illnesses, and medication use, referencing relevant sections of the DD 2766 form for comprehensive medical history insights. Moreover, it emphasizes the importance of dental readiness, immunization records, and other clinical preventive services, ensuring a thorough scrutiny of the service member's health. Objective assessments are captured, including vision acuity and vital signs, coupled with medical equipment needs specific to deployment scenarios. The assessment portion identifies health risks and sets the stage for a personalized plan that underscores preventive measures, medical referrals, and lifestyle counseling tailored to the individual's needs. This document is not just a formality but a critical tool in sustaining the health and operational readiness of those who serve, underlining the military's commitment to its personnel's physical and mental health.
| Question | Answer |
|---|---|
| Form Name | Navmed 6120 4 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | health pha record, 6120 4, periodical health assessment, navmed 6120 |
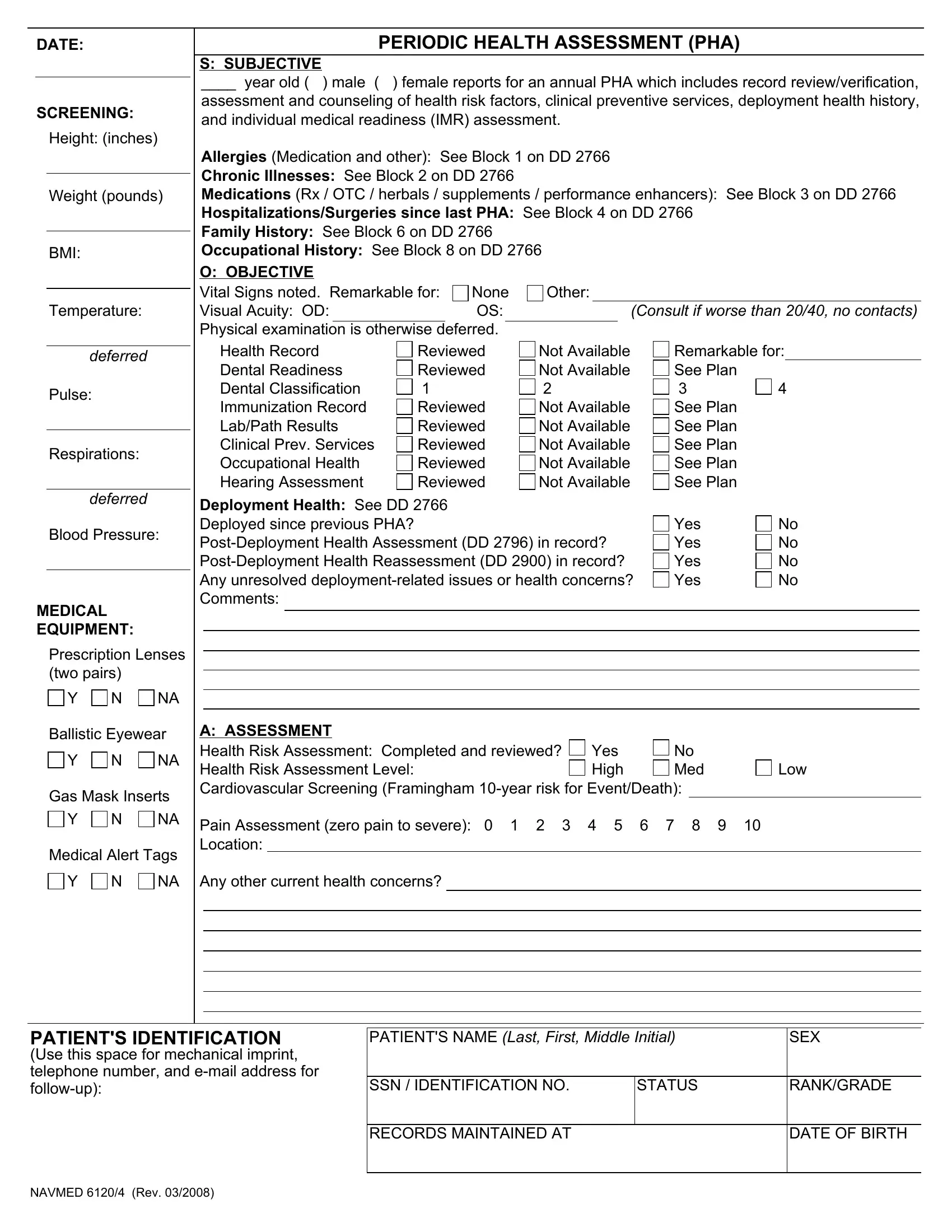
DATE:
SCREENING:
Height: (inches)
Weight (pounds)
BMI:
Temperature:
PERIODIC HEALTH ASSESSMENT (PHA)
S: SUBJECTIVE
____ year old ( ) male ( ) female reports for an annual PHA which includes record review/verification,
assessment and counseling of health risk factors, clinical preventive services, deployment health history, and individual medical readiness (IMR) assessment.
Allergies (Medication and other): See Block 1 on DD 2766
Chronic Illnesses: See Block 2 on DD 2766
Medications (Rx / OTC / herbals / supplements / performance enhancers): See Block 3 on DD 2766
Hospitalizations/Surgeries since last PHA: See Block 4 on DD 2766
Family History: See Block 6 on DD 2766
Occupational History: See Block 8 on DD 2766
O: OBJECTIVE |
|
|
|
Vital Signs noted. Remarkable for: |
None |
Other: |
|
Visual Acuity: OD: |
OS: |
|
(Consult if worse than 20/40, no contacts) |
Physical examination is otherwise deferred.
deferred Pulse:
Respirations:
Health Record
Dental Readiness
Dental Classification
Immunization Record
Lab/Path Results
Clinical Prev. Services
Occupational Health
Hearing Assessment
Reviewed
Reviewed
1
Reviewed
Reviewed
Reviewed
Reviewed
Reviewed
Not Available
Not Available
2
Not Available
Not Available
Not Available
Not Available
Not Available
Remarkable for: See Plan
3 4
See Plan See Plan See Plan See Plan See Plan
deferred
Blood Pressure:
MEDICAL
EQUIPMENT:
Prescription Lenses (two pairs)
Y N NA
Deployment Health: See DD 2766 Deployed since previous PHA?
Yes |
No |
Yes |
No |
Yes |
No |
Yes |
No |
Ballistic Eyewear
Y N NA
Gas Mask Inserts
Y N NA
Medical Alert Tags
Y N NA
A: ASSESSMENT |
|
|
|
Health Risk Assessment: Completed and reviewed? |
Yes |
No |
|
Health Risk Assessment Level: |
High |
Med |
Low |
Cardiovascular Screening (Framingham
Pain Assessment (zero pain to severe): 0 1 2 3 4 5 6 7 8 9 10 Location:
Any other current health concerns?
PATIENT'S IDENTIFICATION
(Use this space for mechanical imprint, telephone number, and
PATIENT'S NAME (Last, First, Middle Initial) |
SEX |
|
|
|
|
SSN / IDENTIFICATION NO. |
STATUS |
RANK/GRADE |
|
|
|
RECORDS MAINTAINED AT |
|
DATE OF BIRTH |
|
|
|
NAVMED 6120/4 (Rev. 03/2008)
PERIODIC HEALTH ASSESSMENT (PHA) (Continued)
Duty Status Assessment |
|
|
|
|
|
|
|
||
On Limited Duty (LIMDU) |
Yes |
No |
NA |
|
Comments: |
|
|
||
Medical Board |
|
Yes |
No |
NA |
|
Comments: |
|
|
|
|
TNPQ |
TNDQ |
NPQ |
LOD |
NA |
|
Comments: |
|
|
P: PLAN / P: PREVENTION |
|
|
|
|
|
|
|
||
1. |
Updated DD 2766 Sections: |
1 |
2 |
3 |
4 |
5 |
6 |
||
2. |
Health counseling performed and documented on the DD 2766: |
Yes |
|
||||||
3. |
Labs ordered for the following: |
Blood Type and RH |
G6PD |
|
|||||
|
Others as required by geographic, occupation, or ISIC |
|
|
||||||
|
Electronic verification complete: |
Yes |
|
No |
|
|
|
||
7
No
HIV
8
9
DNA
10
11
Lipids
4. Immunizations ordered for the following: |
MMR |
|
Tdap (1 time booster) or |
|
Td |
IPV Influenza |
|||||
Hep A #1 #2 |
Hep B #1 |
#2 |
#3 (required for all new recruits) TWINRIX® may be used (3 shots required) |
||||||||
Other immunizations: |
|
|
|
|
|
|
|
|
|
|
|
Electronic verification complete: |
Yes |
|
No |
|
|
|
|
|
|||
5. Tuberculosis Screening:
PPD |
Placement: |
|
Results: |
6. Clinical Preventive Services recommended: |
Pap |
Chlamydia Mammogram |
Colorectal |
|||
Clinical Breast Exam |
Testicular Exam |
Prostate |
Cholesterol |
|
||
Other: |
|
|
|
|
|
|
7. |
Referred to Dental for: |
Annual |
Dental Class 3 |
Dental Class 4 |
|
8. |
Referred to PCM for: |
Physical Fitness Clearance |
|||
|
Current Medications / Supplements |
Chronic Medical Conditions |
|||
|
Other: |
|
|
|
|
Bitewings |
Panograph |
Current Illness / Injury
9. Referred for |
Preventive / Healthy Lifestyle Counseling: |
||
Tobacco |
Use |
Physical Activity |
Safety |
Sexuality |
|
Other |
|
Alcohol Use
Dental Care
Nutrition
Mental Health
10. Other indicated referrals:
Audiology |
Optometry |
Chaplain |
DAPA |
Other: |
|
Behavioral Health
FFSC
OB / GYN Semper Fit
Dietician |
OCC Health |
Weight Management |
|
11. Member readiness reviewed |
Yes |
No and updated in approved electronic data system |
|
Member is fully medically ready and requires no |
No |
||
Yes
No
12. Additional Comments:
13.Member informed that completion of recommended tests / immunizations / screenings is to be performed within the next 30 days, and he/she is personally responsible for maintaining IMR. Service Member received health risk prevention / healthy lifestyle counseling and voiced understanding.
Member Signature: |
|
|
Date: |
|
HM / MDR Signature: |
|
|
Date: |
|
Provider Signature: |
|
|
Date: |
|
|
|
|
|
|
NAVMED 6120/4 (Rev. 03/2008)