It is really straightforward to fill out the nevada application assistance spaces. Our software can make it nearly effortless to fill in any kind of PDF file. Below are the primary four steps you'll want to follow:
Step 1: First, press the orange button "Get Form Now".
Step 2: The file editing page is now open. You can add information or update present content.
These particular areas will frame the PDF template that you'll be creating:
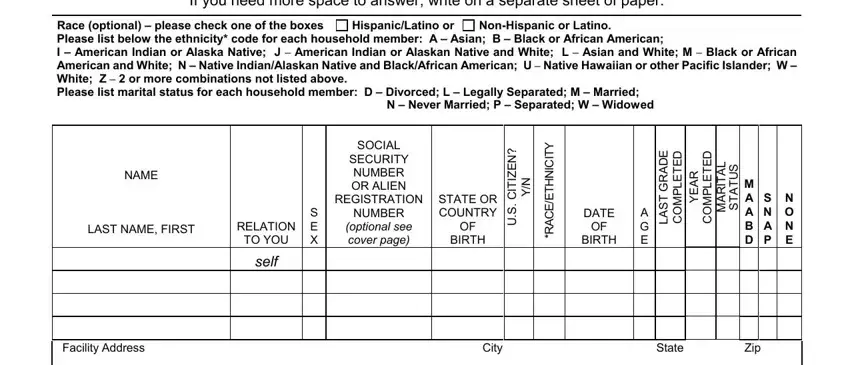
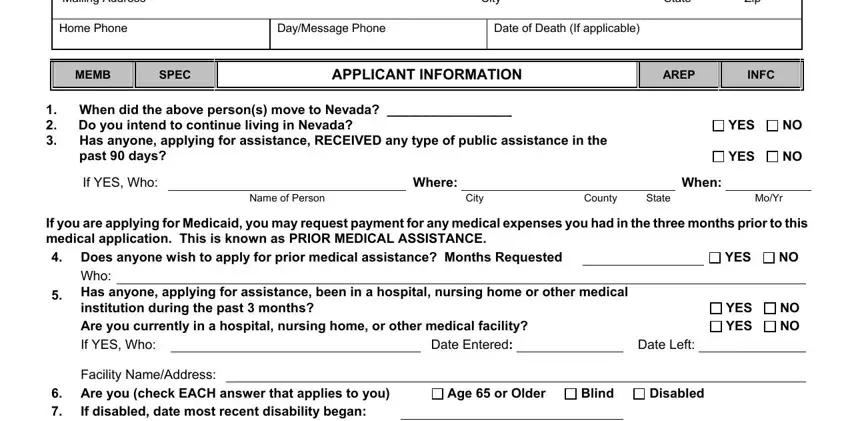
In the Mailing Address, City, State, Zip, Home Phone, DayMessage Phone, Date of Death If applicable, MEMB, SPEC, APPLICANT INFORMATION, AREP, INFC, YES, YES, and When did the above persons move box, type in the information you have.
In the area talking about Under penalty of perjury I swear, Your Signature, Date, and PHOTOCOPY AND DATE STAMP PAGE TO, you are required to type in some vital information.

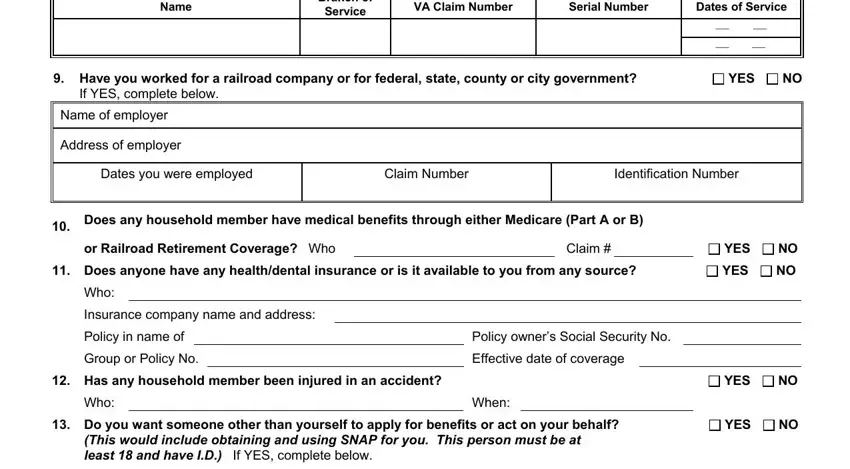
The area Name, Branch of Service, VA Claim Number, Serial Number, Dates of Service, Have you worked for a railroad, YES, If YES complete below, Name of employer, Address of employer, Dates you were employed, Claim Number, Identification Number, Does any household member have, and or Railroad Retirement Coverage Who should be where to include all sides' rights and obligations.
Finish by reviewing the following fields and filling them out accordingly: Who, Telephone Number, Name, Address, Age, RESIDENCE INFORMATION, If you or your spouse reside in a, Is this residence occupied by a, Do you receive rental income from, What is the fair market value of, nd Mortgage, PROP, YES, YES, and YES.
Step 3: Select the "Done" button. Now you can transfer the PDF form to your electronic device. Additionally, you'll be able to send it via email.
Step 4: Attempt to generate as many copies of your file as possible to prevent potential problems.
