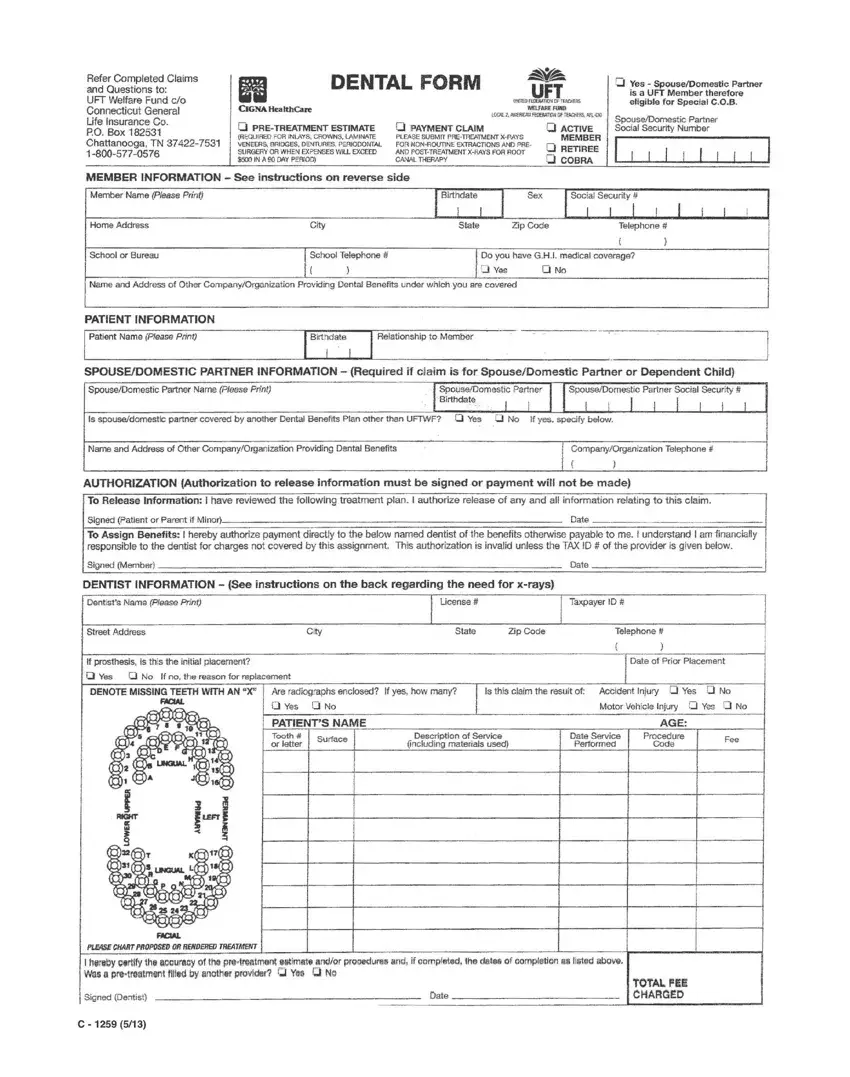
Managing dental health is a crucial aspect of overall well-being, and for members of the United Federation of Teachers (UFT), the UFT Welfare Fund Contact form serves as a vital tool in facilitating this care. Designed to streamline the process of submitting dental claims, this document is directed to the UFT Welfare Fund under the care of Connecticut General Life Insurance Co., located in Chattanooga, TN. It covers a range of options, including payment claims and pre-treatment estimates, emphasizing the necessity of prior submissions for procedures like inlays, crowns, and dentures when the anticipated expenses exceed a certain threshold within a 90-day period. The form meticulously collects member information, including eligibility for Global Health & Life (G.H.L) medical coverage, spouse or domestic partner's details, and other insurance coverage, ensuring a comprehensive understanding of the member's coverage ecosystem. Authorization sections underscore the importance of permission to release information for claims processing and direct payment to dentists, thus highlighting a member-focused approach. Additionally, dentist information, crucial for the claim, emphasizes the professional's credentials and service details, providing a clear path for members in managing their dental health needs efficiently.
| Question | Answer |
|---|---|
| Form Name | Uft Welfare Fund Contact |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | uft cigna dental, uft dental, uft dental form pdf, uft 1259 dental form |
