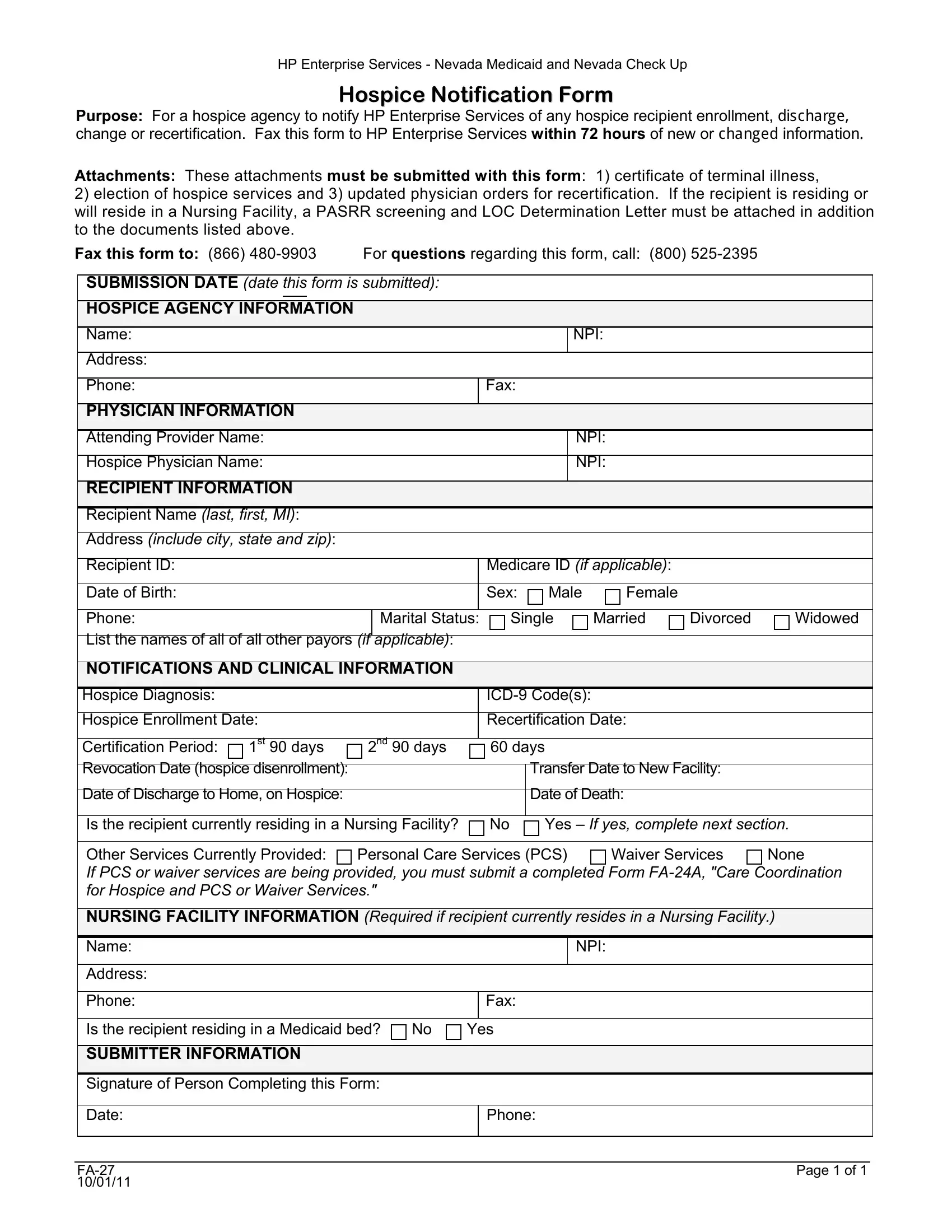
In the realm of healthcare administration within Nevada, the Nevada FA-27 form plays a crucial role in the operational procedures of hospice agencies. This specific document serves as a notification tool for HP Enterprise Services, the entity tasked with managing both Nevada Medicaid and Nevada Check Up, regarding key hospice recipient details. These include enrollment in hospice care, any significant changes therein, discharge, and recertification statuses. To maintain compliance and facilitate timely updates, hospice agencies are mandated to transmit this form within a 72-hour window following any new information or alterations. Accompanying the FA-27 form, crucial attachments are required for a comprehensive submission: notably, a certificate signifying terminal illness, an affirmative election of hospice services by the recipient, and, for instances of recertification, up-to-date physician orders. Furthermore, should the recipient be situated or projected to reside within a Nursing Facility, additional documentation—namely, a PASRR screening and a Letter of the Level of Care Determination—becomes imperative for attachment, underscoring the form’s significance in ensuring meticulous coordination of care. Directed to HP Enterprise Services through specified fax communication, the form is accompanied by a designated contact number, ensuring clarity and support for hospice agencies navigating the submission process. This systematic approach underscores the form's pivotal role in streamlining hospice care management, ensuring compliant, coordinated, and continuous care for those with terminal illnesses within the state of Nevada.
| Question | Answer |
|---|---|
| Form Name | Nevada Form Fa 27 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | HP, NPI, ICD-9, Revocation |
HP Enterprise Services - Nevada Medicaid and Nevada Check Up
Hospice Notification Form
Purpose: For a hospice agency to notify HP Enterprise Services of any hospice recipient enrollment, GLVFKDUJH change or recertification. Fax this form to HP Enterprise Services within 72 hours of new or FKDQJHG LQIRUPDWLRQ
Attachments: These attachments must be submitted with this form: 1) certificate of terminal illness,
2)election of hospice services and 3) updated physician orders for recertification. If the recipient is residing or will reside in a Nursing Facility, a PASRR screening and LOC Determination Letter must be attached in addition to the documents listed above.
Fax this form to: (866) |
For questions regarding this form, call: |
(800) |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
SUBMISSION DATE (date this form is submitted): |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
HOSPICE AGENCY INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
NPI: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
|
|
|
|
|
|
Fax: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
PHYSICIAN INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Attending Provider Name: |
|
|
|
|
|
|
|
|
NPI: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Hospice Physician Name: |
|
|
|
|
|
|
|
|
NPI: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
RECIPIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recipient Name (last, first, MI): |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Address (include city, state and zip): |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Recipient ID: |
|
|
|
|
|
|
|
|
|
Medicare ID (if applicable): |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Date of Birth: |
|
|
|
|
|
|
|
|
|
Sex: |
Male |
Female |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Phone: |
|
|
|
|
|
Marital Status: |
|
Single |
Married |
Divorced |
Widowed |
||||
|
List the names of all of all other payors (if |
|
applicable): |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
NOTIFICATIONS AND CLINICAL INFORMATION |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hospice Diagnosis: |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Hospice Enrollment Date: |
|
|
|
|
|
|
Recertification Date: |
|
|
||||||
|
Certification Period: |
1st 90 days |
2nd 90 days |
|
|
60 days |
|
|
|
|||||||
|
|
|
|
|
|
|||||||||||
|
Revocation Date (hospice disenrollment): |
|
|
|
|
|
|
|
Transfer Date to New Facility: |
|
||||||
|
|
|
|
|
|
|
|
|
||||||||
|
Date of Discharge to Home, on Hospice: |
|
|
|
|
|
|
|
Date of Death: |
|
|
|||||
|
|
|
|
|
|
|||||||||||
|
Is the recipient currently residing in a Nursing Facility? |
|
|
No |
Yes – If yes, complete next section. |
|||||||||||
|
|
|
|
|
||||||||||||
|
Other Services Currently Provided: |
Personal Care Services (PCS) |
Waiver Services |
None |
||||||||||||
|
If PCS or waiver services are being provided, you must submit a completed Form |
|||||||||||||||
|
for Hospice and PCS or Waiver Services." |
|
|
|
|
|
|
|
|
|
||||||
|
|
|||||||||||||||
|
NURSING FACILITY INFORMATION (Required if recipient currently resides in a Nursing Facility.) |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
NPI: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
|
|
|
|
|
|
Fax: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Is the recipient residing in a Medicaid bed? |
No |
Yes |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
SUBMITTER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of Person Completing this Form: |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Date: |
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 1 of 1 |
|
0/01/11 |
|